The urinary system is the Rodney Dangerfield of the body: it gets no respect. Medical doctors pay worship to the cardiovascular and nervous systems; alternative healers pay homage to the colon and practice ancient detoxing rites. But who thinks about the urinary system? Who pays attention to the kidneys until something goes wrong? And make no mistake, things go wrong. When it comes to the urinary system, we’re not just talking about kidney stones and kidney failure, which affect millions of people in the United States alone, but more significantly kidney sludge, which compromises kidney function in virtually every adult living in a first world country. And we’re also talking about infection and inflammation in the urinary tract, not to mention incontinence in the bladder.
In this series of newsletters on the urinary system, we will examine not only the anatomy and physiology of the kidneys, but also the ureters (which convey waste from the kidneys), and the bladder (which stores waste until it can be excreted). But more importantly, we will use our newfound understanding of how everything works to explore those things that can go wrong in all areas of the system — some life threatening, and some merely compromising of life quality — and how we can use natural therapies to overcome those problems.
Background
The National Kidney and Urologic Diseases Information Clearinghouse estimates that each year more than 100,000 Americans are newly diagnosed with kidney failure. More than a half million currently have End Stage Renal Disease (ESRD), and an astounding 20 million have physiological evidence of chronic kidney disease.1 “Kidney and Urologic Diseases Statistics for the United States.” National Kidney & Urologic Diseases Information Clearinghouse (NKUDIC). (Accessed 3 Mar 2012.) <http://kidney.niddk.nih.gov/KUDiseases/pubs/kustats/index.aspx> The United States has the highest incident rate of ESRD in the world, followed by Japan. As per NHANES III (Third National Health and Examination Survey), the prevalence of chronic kidney disease is a mind numbing 37.8% among patients older than 70 years.2 Pradeep Arora. “Chronic Kidney Disease.” Medscape Reference. Updated 16 Feb 2012. (Accessed 3 Mar 2012.) <http://emedicine.medscape.com/article/238798-overview#a0156> And that’s just in America. Internationally, the incidence rates of end-stage renal disease (ESRD) have increased steadily since 1989.
But it’s not just End Stage Renal Disease. Kidney stones, one of the most painful conditions known to man, have beset humans for centuries. Scientists have found evidence of kidney stones in a 7,000-year-old Egyptian mummy. Unfortunately, kidney stones are one of the most common disorders of the urinary tract. Each year, people make almost 3 million visits to health care providers in the United States alone and more than half a million people go to emergency rooms for kidney stone problems.3 “Kidney Stones in Adults.” National Kidney & Urologic Diseases Information Clearinghouse (NKUDIC). (Accessed 3 Mar 2012.) <http://kidney.niddk.nih.gov/kudiseases/pubs/stonesadults/> And worldwide the incidence of kidney stones, although less than that of the U.S. and Japan, has been steadily increasing.4 Victoriano Romero, Haluk Akpinar, and Dean G Assimos. “Kidney Stones: A Global Picture of Prevalence, Incidence, and Associated Risk Factors.”Victoriano Romero, Haluk Akpinar, and Dean G Assimos. “Rev Urol. 2010 Spring-Summer; 12(2-3): e86–e96. <http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2931286/>
And then, as we move on down the urinary tract, we find disturbingly high levels of conditions such as:
- Interstitial cystitis
- Urinary tract infections
- Incontinence
According to a 2009 Rand study, as many as 8 million women in the U.S., or 3% of all U.S. women, suffer from interstitial cystitis and suffer from debilitating symptoms.5 Sandra H. Berry, Marc N. Elliott, Marika Suttorp, Laura M. Bogart, et al. “Prevalence of Symptoms of Bladder Pain Syndrome/Interstitial Cystitis Among Adult Females in the United States.” I, v. 186, no. 2, Aug. 2011, p. 540-544. <http://download.journals.elsevierhealth.com/pdfs/journals/0022-5347/PIIS0022534711035452.pdf> And although the incidence in men is less, it is still afflicts over 1.5 million men in the U.S. alone.6 Clemens JQ, Meenan RT, Rosetti MC, Gao SY, Calhoun EA. “Prevalence and incidence of interstitial cystitis in a managed care population.” J Urol. 2005 Jan;173(1):98-102; discussion 102. <http://www.ncbi.nlm.nih.gov/pubmed/15592041> Urinary tract infections (UTIs) are considered to be the most common bacterial infection. Statistically, almost half of all women will experience one UTI during their lifetime.7 Foxman B. “Epidemiology of urinary tract infections: incidence, morbidity, and economic costs.” Am J Med. 2002 Jul 8;113 Suppl 1A:5S-13S. <http://www.ncbi.nlm.nih.gov/pubmed/12113866> Approximately 75 percent of all women can look forward to experiencing at least one vaginal yeast infection during their lifetimes.8 “Vaginal Yeast Infections.” I. (Accessed 3 Mar 2012.) <http://www.obgynvirginia.com/conditions_And_Treatments/yeast-infections.php> And as for urinary incontinence, most studies report some degree of urinary incontinence in 25-45% of women and 11-34% of older men.9 Buckley BS, Lapitan MC; Epidemiology Committee of the Fourth International Consultation on Incontinence, Paris, 2008. “Prevalence of urinary incontinence in men, women, and children–current evidence: findings of the Fourth International Consultation on Incontinence.” I. 2010 Aug;76(2):265-70. Epub 2010 Jun 11. <http://www.ncbi.nlm.nih.gov/pubmed/20541241>
Make no mistake, the urinary system may be treated like Rodney Dangerfield, but its impact on our lives is a lot more like Rambo.
The urinary system
 The colon and the urinary system are like yin and yang. They are polar opposites, but at their cores, they share common purpose. Whereas the colon is primarily responsible for excretion, with a secondary function of conserving water, the urinary system is all about preserving homeostasis through conserving water and electrolytes, with a secondary function of excreting toxins. It is composed of the kidneys, ureters, bladder, and urethra. The kidneys are the primary filtering and rebalancing organs in the body. The ureters are the conduits to the bladder from the kidneys. And the bladder stores urine and waste until it is convenient and socially acceptable to dispose of them — unless you’ve had too much stout to drink and you’re caught far away from the loo. In addition, by virtue of its ability to regulate homeostasis, the urinary system also plays a major role in regulating some of the body’s most important systems. For example, the urinary system is a primary player in maintaining blood volume, normal blood pressure, normal blood composition, and normal body and blood pH. And if that weren’t enough, it also synthesizes and secretes calcitrol, the hormonally active form of vitamin D used by the body to regulate blood levels of calcium, and erythropoietin, a hormone that promotes the formation of red blood cells in the bone marrow.
The colon and the urinary system are like yin and yang. They are polar opposites, but at their cores, they share common purpose. Whereas the colon is primarily responsible for excretion, with a secondary function of conserving water, the urinary system is all about preserving homeostasis through conserving water and electrolytes, with a secondary function of excreting toxins. It is composed of the kidneys, ureters, bladder, and urethra. The kidneys are the primary filtering and rebalancing organs in the body. The ureters are the conduits to the bladder from the kidneys. And the bladder stores urine and waste until it is convenient and socially acceptable to dispose of them — unless you’ve had too much stout to drink and you’re caught far away from the loo. In addition, by virtue of its ability to regulate homeostasis, the urinary system also plays a major role in regulating some of the body’s most important systems. For example, the urinary system is a primary player in maintaining blood volume, normal blood pressure, normal blood composition, and normal body and blood pH. And if that weren’t enough, it also synthesizes and secretes calcitrol, the hormonally active form of vitamin D used by the body to regulate blood levels of calcium, and erythropoietin, a hormone that promotes the formation of red blood cells in the bone marrow.
Let’s begin our exploration of the urinary system by taking a macro view of the organs.
Kidneys
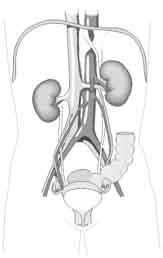
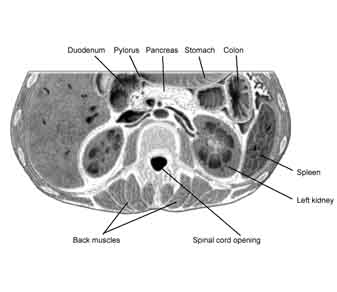
Position-wise, the kidneys are paired organs lying to the right and left of the spinal column. They are entirely retroperitoneal, which is to say they sit behind the peritoneum (the tissue that lines the abdominal wall and covers most of the organs in the abdomen). Since it is pushed down by the liver, the right kidney (the left side in most illustrations) sits lower than the left kidney. Curiously, the kidneys do not parallel the back, but actually angle in towards the belly button. This allows them to take advantage of the natural protection offered by the backbone and the big muscles that run along the spine, since the kidneys actually nestle in against those anatomical elements.
Although the kidneys themselves are permeated with a vast arterial network, required as we will see to support their functions, they are nevertheless each supplied by only one pair of blood vessels (the right and left renal arteries and veins). This leads to a curious contradiction. With only one blood vessel leading in and out, it makes each kidney easy to remove or transplant. On the other hand, because each kidney contains so many blood vessels internally, any wound to the kidney causes profuse bleeding and is difficult to repair. In other words, replacement is easy, but surgery on the organ itself is extremely difficult — although skilled surgeons can remove diseased sections of a kidney because there is so much internal collateral circulation.
The kidneys are vital organs. You need at least one to survive. Fortunately, because they are so vital, your body has built in redundancy. Not only can you survive on just one kidney, but if you lose kidney function, up to a point, the kidneys have the ability to transfer more load to the remaining parts that are still functioning. If, on the other hand, your kidneys totally shut down, you will die…but not instantly. You can survive for 2-4 days after total kidney failure. This time lag allows for hemodialysis, about which we will talk more later. The key point to understand for now is that because you don’t die instantly without kidney function, it allows patients to come to a dialysis center just 2-3 times a week instead of having to be hooked up to a dialysis machine 24/7.
As we mentioned already, the primary function of the kidneys is not to excrete waste like the colon, but to maintain balance and internal stability in the body by cleansing the blood. The medical term for balance is homeostasis — or as the astronauts say in The Right Stuff, “to maintain an even strain.” Basically, the kidneys take everything except blood cells (red and white) that pass through them and filter it out. Then they pick up signals from the body telling them what needs to be actually eliminated from the body and what needs to be preserved to maintain homeostasis. Then based on these internal signals, they put everything that’s required back into the system. Everything else is excreted in the urine. Or to explain it another way, the kidneys work using a two step process. In step one, they remove everything from the blood. In step two, based on signals from the brain and body, they reabsorb all necessary components in the quantities required to achieve balance. The signals come from receptors that track everything from dissolved bio-chemicals to blood pressure, from pulse to temperature, and much more.
Things that the kidneys filter and regulate include waste, solutes, toxins, proteins, amino acids, water, electrolytes, and parts of the pH buffering system — notably bicarbonate. They also recycle necessary elements and maintain normal blood volume, blood pressure, normal blood composition, and blood and body pH. And as already been mentioned, they synthesize calcitrol for bone building and erythropoietin for production of red blood cells.
The anatomy of the kidneys
As we explore the anatomy of the kidney, we’re going to hear a number of words that begin with “renal-” and “nephro-.” In fact, they both mean kidney. Renal comes from the Latin “renes,” and nephro from the Greek “nephros.” Think nephrologist and renal failure. They both mean kidney. There is no difference. Incidentally, the word “kidney” itself comes from England during the Middle Ages. Think Chaucer.
That said, the outer layer of the kidney is called the renal cortex. The inner layer is called the renal medulla. To help remember them: cortex comes from the Latin word for “bark” as in the bark of a tree — thus it refers to the outer layer of an organ. Medulla also comes from the Latin and refers to the pith or marrow of something — thus its inner layer.
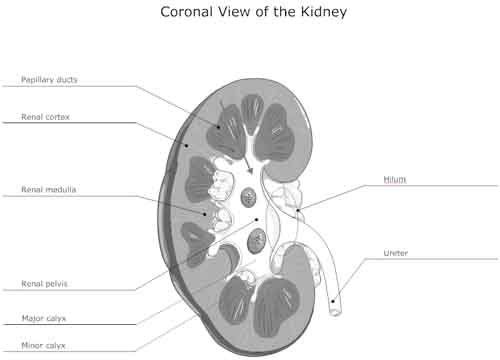
The renal medulla consists of 10-15 medullary pyramids. The inside or medial tip of each pyramid is called the renal papilla. Papilla is the Latin word for nipple, which is less for what it looks like and more for what it functions as –urine that is collected by the kidney passes through the papillae on its way out through the ureter. So far, it doesn’t matter whether or not you remember any of these terms. All that matters is that you get the general lay of the land so that we can refer back to it as needed.
The renal pelvis can be thought of as the collection area of the kidney, where the urine gathers after coming out of the different papillary ducts on its way into the dilated funnel part of the ureter, where it nestles inside the kidney. The renal pelvis is composed of calycses (“cups”) — both minor calyces (aka renal papilla) and major calyces. In effect, the renal pelvis is the first collecting system in the kidney. Once the urine has been squeezed out of the cortex and medulla into the pelvis, it is never modified again. From the renal pelvis, it goes through the ureter, pushed along by gravity and peristalsis, and then into the bladder, where it is collected for the final time, waiting for an appropriate moment to be voided from the body. The renal hilum (or hilus) is the entry/exit way for the blood vessels that feed the kidney and the ureter.
Again, so far, nothing is crucial to remember, unless you’re preparing for an anatomy test, other than having a general sense of how things lay out in the kidneys.
But that’s about to change. We’re now going to touch on the microscopic anatomy of the kidney. That’s where the important stuff happens — the stuff you need to know about so you can understand how to avoid problems and make the urinary system work better. For now, we’re only going to touch on the micro-anatomy, saving a detailed discussion for the next newsletter.
Kidneys — microscopic anatomy
The nephron is the major functioning unit of the kidney, and there are approximately one million of them in each kidney. Considering that each kidney is about the size of a fist, that should give you an idea of how small a nephron actually is. And here is our first crucial point to remember: you are born with your total complement of nephrons. No new ones can ever be formed — ever. You can never regenerate lost capacity. It is true, however, as I mentioned earlier, that the loss of nephrons can compensated for without new ones being formed because the kidneys can redistribute workload — but again, only up to a point. For example, if you remove one kidney, the nephrons in the remaining kidney will increase their workload to make up the difference. That is why you can survive with just one kidney; that is why you can donate a kidney.
But this ability to compensate is not infinite. There is a limit, and as you cross that limit through the plugging up of nephrons with kidney sludge or the killing of nephrons from diabetes, you will start to get sicker and sicker as you progressively lose kidney function. Therefore, it is vital that you keep as much kidney function as possible as you age and that you maximize the ability of nephrons to perform at peak levels for as long as possible. As we proceed, we will explicitly explore how that can be done.
Nephron composition and function
The nephrons are the heart and soul of the kidney. They are the functional filters that make everything work. In non-technical terms, a nephron consists of the blood vessels that carry blood into and out of the nephron, a ball where the primary filtering takes place, and a series of tubules and ducts that both finish the filtering and then reverse direction and pump important bio-chemicals back into the bloodstream to achieve homeostasis. There are actually two different kinds of nephrons in the kidneys. Juxtamedullary nephrons have much longer descending and ascending loops of Henle and thus extend far deeper into the renal medulla than normal nephrons. Their function is to fine-tune blood composition. But given that difference, all nephrons function in the same way.
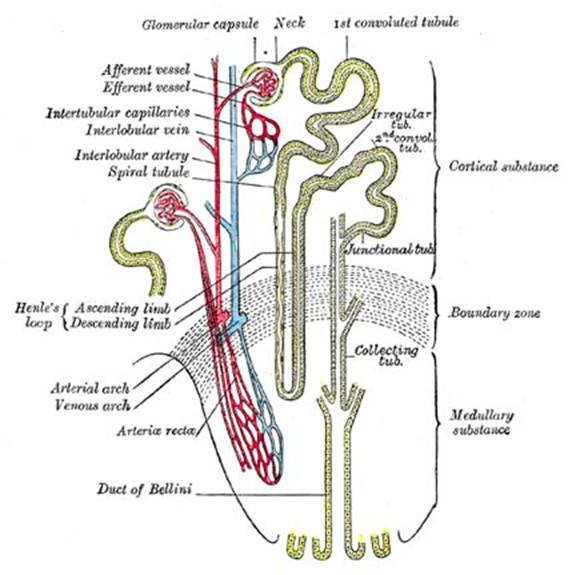
The blood vessel entering the nephron is known as the afferent arteriole, and the blood vessel leaving it is known as the efferent arteriole. Afferent means moving inward, and efferent means moving outward — easy to remember, but not important to worry about. The renal corpuscle is composed of an afferent arteriole, the glomerulus (“little ball”), and an efferent arteriole. You can think of it as the filtering component of the nephron. The one term you will want to remember out of all of this is “glomerulus” (pronounced: gloh-mer-yuh-luhs), which is essentially a group of capillaries bunched up into a little ball. The ball is covered in a double layer of epithelium, called the Bowman’s capsule. Put everything together — the glomerulus, the Bowman’s capsule, and the afferent and efferent arterioles — and you have what’s called the renal corpuscle (AKA, the glomerular capsule). Filtration works as follows.
- Blood runs through the arterioles of the glomerulus. Pretty much everything except blood cells pass out of the arterioles and into the Bowman’s capsule, passing into the “proximal convoluted tubule” (labeled 1st convoluted tubule in the illustration above) which sits immediately next to the glomerular capsule. This is the first stage of urine production. Let’s now look at exactly how the blood is filtered by the arterioles in the glomerulus and “pre-urine” is pushed into the Bowman’s capsule.
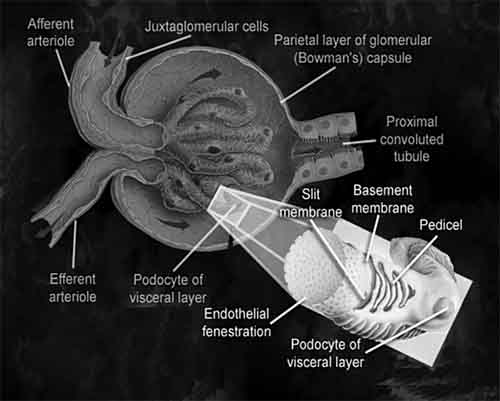
- The endothelium of the glomerular capillaries is riddled with small holes (endothelial fenestration) that pretty much allow everything other than red and white blood cells to pass into the Bowman’s capsule. In other words, we can now make a simple health observation: blood in the urine is never normal.
- Problems associated with blood in the urine include inflammation of the glomerulus, kidney stones which rough up the walls of the ureter or the tissue of the renal pelvis, external blows to the kidney, and inflammation of the bladder.
- The basement membrane has even smaller holes than the endothelial layer, which are designed to trap large proteins and keep them in the blood.
- A third filtration layer inside the glomerulus, the podocytes (“foot cells”) have yet again smaller holes that trap even smaller proteins and amino acids but allow ions (such as sodium and potassium ions) to pass into the urine collection system. The net result is that fluid entering the proximal convoluted tubule should then be free of blood cells, proteins, and other large molecules. And that’s why urinary dipsticks check for sugar, blood, and proteins — none of which should be in your urine.
- Once this “pre-urine” leaves the capsule, it passes into the proximal convoluted tubule, which although still part of the nephron, represents the first stage in the urine collection system. The tubule is lined with blood vessels that reabsorb nutrients, essential bio-chemicals, and ions back from the urine and into the bloodstream, while at the same time allowing for the blood to excrete additional waste into the urine.
- From the proximal tubule, the “pre-urine” travels down the loop of Henle and back up the other side to the distal convoluted loop, undergoing further balancing and exchanges all along the way. Once through the 2nd convoluted tubule, it is now full-fledged urine, which passes into the collecting tube, where it joins with urine from other nephrons — then through the papillary duct, into the renal pelvis, and on out of the kidney through the ureter.
- Or to look at it another way, all filtering is done in the glomerulus. After that, it’s all about adjusting balance.
The following video summarizes everything we’ve talked about so far.
In our next issue of the newsletter, we will examine the functioning of the nephrons in more detail and explore some of the things that can go wrong. For now, let’s continue looking at the rest of the urinary system.
Ureters
Once urine has been filtered and fine tuned in the nephrons, it passes through the renal pelvis and enters the right and left ureters — one for each kidney. The ureters then pass out of the kidneys through the renal hilus and run parallel to the spinal column as they make their way down the body to the bladder. The ureters are approximately 30 cm (12 inches) long and 5 mm (3/16 of an inch) in diameter. Urine moves through the ureters both as the result of gravity and peristalsis. This makes it possible for astronauts to spend prolonged time in weightlessness — otherwise they wouldn’t be able to urinate. The ureters enter the bladder through what is known as the trigone. The trigone is a smooth triangular region of the bladder formed by the two ureteral orifices and the internal urethral orifice. It forms a functional (not anatomical) valve to prevent urine reflux.
Bladder
The bladder is located in the midline behind the pubis. It is located in front of the rectum in the male and in front of the uterus in the female. It has an internal sphincter, which is involuntary, and an external sphincter, which is voluntary. The area is very sensitive to expansion and once stretched to a certain degree, the urinary bladder signals the brain of its need to empty. The signals become stronger, as you are probably well aware, as the bladder continues to fill.
Urethra
The urethra exits from the bladder. It is short in women and longer in men — having further to travel. The shorter length of the female urethra makes incontinence and bladder infections more common in women.
Problems and solutions
Although kidney stones primarily inflict their pain and damage when passing through the ureters, they are created in the kidneys, so we will save our discussion of them for later in our series. For now, we will focus our discussion on
- Urinary tract infection
- Inflammation — Interstitial cystitis
- Incontinence
Urinary tract infection
Since urine is filtered out from blood, which is normally sterile, urine straight from the kidneys is also normally sterile. That said, it is worth noting that urine contains things such as minerals and sugar, if you’re diabetic, that would help promote the growth of bacteria if they were present. So where can bacteria come from?
If you have a systemic infection, it is possible for that infection to make its way through the kidneys and down into the ureter and bladder; however, that is rare as it requires an extensive bacterial infection in the bloodstream to make its way through the kidney’s filters. Far more common is for infection to make its way up — through the urethra and into the bladder. Since women have a shorter urethra than men, this makes them more prone to urinary tract infections. In addition, they are anatomically more prone to transferring E. coli from the rectum into the urethra while cleaning. But even then, the body has defenses.
First, if you are well populated with beneficial bacteria (probiotics) they are likely to have migrated into your urinary tract — lining it and protecting it from invading E. coli. In addition, the two bladder sphincters form a highly effective barrier to prevent bacteria from making their way from the urethra into the bladder. And then the trigones help prevent any bacteria in the bladder from making their way up into the ureters. And finally the frequent passage of urine down the ureter, through the bladder, and out the urethra tends to flush any bacteria that make it through these defenses. The bottom line is that it’s difficult for bacteria to make their way up through the urinary system…but not impossible. And the problem can be exacerbated by things such as dehydration so that you don’t have sufficient urinary flush pushing the bacteria down, weak pelvic muscles which prevent the sphincters from closing tightly, dysbiosis so that you don’t have a full complement of probiotics lining your urinary tract, and sloppy cleansing habits that continually expose the urethra to E. coli bacteria.
Men, however, have a different problem. As they age and their prostates enlarge, it tends to squeeze the urethra, which makes it harder to completely void the bladder. This allows urine to sit around longer in the bladder, which gives it more time to acquire an infection and serve as a medium for its growth.
Natural treatments for urinary tract infections include:
- An antipathogenic formula that contains things like garlic, oil of oregano, and olive leaf extract, to pass through the digestive tract and into the bloodstream and kidneys to directly take on the infection.
 Cranberry juice: The consumption of cranberry juice has been recommended for the prevention of urinary tract infections, and a 1994 clinical study provides scientific validation of this claim.10 Avorn J, Monane M, Gurwitz JH, Glynn RJ, Choodnovskiy I, Lipsitz LA. “Reduction of bacteriuria and pyuria after ingestion of cranberry juice.” JAMA 1994;271:751-754. <http://jama.ama-assn.org/content/271/10/751.abstract> However, it seems the effect is due not to the highly acidic nature of cranberries, as once supposed, but to specific compounds in cranberries that inhibit the adherence of Escherichia coli to uroepithelial cells.11 Zafriri D, Ofek I, Adar R, Pocino M, Sharon N. “Inhibitory activity of cranberry juice on adherence of type 1 and type P fimbriated Escherichia coli to eucaryotic cells.” Antimicrob Agents Chemother 1989;33:92-98. <http://www.ncbi.nlm.nih.gov/pmc/articles/PMC171427/> ,12 Ofek I, Goldhar J, Zafriri D, Lis H, Adar R, Sharon N. “Anti-Escherichia coli adhesin activity of cranberry and blueberry juices.” N Engl J Med 1991;324:1599-1599. <http://www.nejm.org/doi/full/10.1056/NEJM199105303242214>
Cranberry juice: The consumption of cranberry juice has been recommended for the prevention of urinary tract infections, and a 1994 clinical study provides scientific validation of this claim.10 Avorn J, Monane M, Gurwitz JH, Glynn RJ, Choodnovskiy I, Lipsitz LA. “Reduction of bacteriuria and pyuria after ingestion of cranberry juice.” JAMA 1994;271:751-754. <http://jama.ama-assn.org/content/271/10/751.abstract> However, it seems the effect is due not to the highly acidic nature of cranberries, as once supposed, but to specific compounds in cranberries that inhibit the adherence of Escherichia coli to uroepithelial cells.11 Zafriri D, Ofek I, Adar R, Pocino M, Sharon N. “Inhibitory activity of cranberry juice on adherence of type 1 and type P fimbriated Escherichia coli to eucaryotic cells.” Antimicrob Agents Chemother 1989;33:92-98. <http://www.ncbi.nlm.nih.gov/pmc/articles/PMC171427/> ,12 Ofek I, Goldhar J, Zafriri D, Lis H, Adar R, Sharon N. “Anti-Escherichia coli adhesin activity of cranberry and blueberry juices.” N Engl J Med 1991;324:1599-1599. <http://www.nejm.org/doi/full/10.1056/NEJM199105303242214> - D-mannose is one of the active ingredients in cranberry juice. It is a naturally occurring simple sugar, close to glucose. Small amounts of D-mannose are metabolized by our bodies; more than small amounts are excreted promptly into the urine. To understand how D-mannose works, you need to understand how E. coli bacteria make their way up the urinary tract. As it turns out, the “cell walls” of each E. coli are covered with tiny fingerlike projections. The very tips of these projections are an amino acid-sugar complex, a “glycoprotein” also called a “lectin.” E. coli “lectins” have the unfortunate capability of “sticking” the bacteria to the inside walls of our bladders and urinary tracts, so they can’t easily be rinsed out by urination. However, D-mannose “sticks” to E. coli lectins even better than E. coli lectins “stick” to human cells. When we take a large quantity of D-Mannose, almost all of it spills into the urine through our kidneys, literally “coating” any E. coli present so they can no longer “stick” to the inside walls of the bladder and urinary tract. The E. coli are literally rinsed away with normal urination! Supplementing with pure D-mannose is more effective than drinking cranberry juice.
- Probiotics are less effective at actually getting rid of urinary tract infections than they are at preventing it in the first place. L. acidophilus is the primary beneficial bacteria in the vaginal tract. When the presence of acidophilus is compromised, this allows the bad guys such as Gardnerella vaginalis or E. coli or Chlamydia to take over. This is particularly important to women to help prevent a whole range of vaginal and urinary tract infections. If you have a sufficient population of acidophilus in your intestinal tract, it will migrate over into the urinary tract and function as a protective barrier.
For a complete protocol for dealing with a urinary tract infection, check out: Urinary Tract Infections, Kidney Health.
Inflammation- interstitial cystitis
Interstitial cystitis (IC) is a painful condition caused by inflammation of the tissues of the bladder wall. Although it is often diagnosed as a sexually transmitted disease, bladder cancer, and bladder infections, its actual cause is unknown. It is frequently misdiagnosed as a urinary tract infection — although its trigger may be connected. Unfortunately, patients can often go years without a correct diagnosis. IC generally occurs around age 30 to 40, although it has been reported in younger people. Women are 10 times more likely to have IC than men.
Because IC varies so much in symptoms and severity, most researchers believe that it may actually be several diseases. One theory being studied is that IC is an autoimmune response following a bladder infection. Another theory is that there are substances in urine which are irritating to people with IC. And still other theories are being studied. Interstitial cystitis is different from urinary tract infections, which are caused by bacteria and can be treated with antibiotics. Studies have shown that antibiotics are not useful for treating IC.
With that said, we can see that the Baseline of Health® approach is more likely to have results than most any other approach since it addresses so many possible causes. For example:
- Raising pH can help by reducing the acidity of the urine. There are a number of ways to do this. Coral calcium and/or potassium drops will work as well as any of them. Ideally, urine should be slightly acidic. Any levels below 5.5 start to present serious health risks.
- Using proteolytic enzymes between meals can help clear up circulating immune complexes, which can promote autoimmune conditions. Another advantage to using a solid detoxing regimen of proteolytic enzymes is that it can actually help reduce the scar tissue in the bladder that is so often a contributing factor in the discomfort of IC.
- Also, using L. carnosine and cetyl-myristoleate can help modulate immune responses.
- Using a strong systemic antioxidant formula can help repair damage to internal tissue.
- DMSO is the only FDA-approved bladder instillation drug for interstitial cystitis. It helps relax the bladder and alleviate pain and inflammation. Some research suggests that more than half of patients improve after six weeks of once-a-week treatments.
Again, think Baseline of Health rather than magic bullets. With that said, one shot you may want to try is using a good kidney stone formula — just in case small kidney stones are contributing to the problem. If that is an issue, the right formula can help in 2-3 days. (We’ll talk more about this next newsletter.)
Note: one other thing you will want to check on is if you are suffering from a hormonal allergy to either estrogen or progesterone. It should not be a surprise that hormones might be involved. 90% of all IC sufferers are women.
Incontinence
 Urinary incontinence is the loss of bladder control. It is more common than you might believe. It is no accident that Depend® sales top $250 million a year or that protective underwear as a whole is cited as the fastest growing dollar volume product in drugstore outlets.13 “Kimberly-Clark – Depend Protective Underwear.” Centerbrain. (Accessed 6 Mar 2012.) <http://www.centerbraininc.com/success/kimberly-clark.php> Moderate to severe incontinence actually affects as many as 3-17% of all women — although the older you are, the higher the incidence. For men it’s about half that at 3-11%. The severity of urinary incontinence ranges from occasionally leaking urine when you cough or sneeze to having an urge to urinate that’s so sudden and strong you don’t get to a toilet in time.14 Victor W Nitti. “The Prevalence of Urinary Incontinence.”Rev Urol. 2001; 3(Suppl 1): S2–S6. <http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1476070/> It can be caused by everyday habits, underlying medical conditions, or physical problems. And it can be temporary or chronic.
Urinary incontinence is the loss of bladder control. It is more common than you might believe. It is no accident that Depend® sales top $250 million a year or that protective underwear as a whole is cited as the fastest growing dollar volume product in drugstore outlets.13 “Kimberly-Clark – Depend Protective Underwear.” Centerbrain. (Accessed 6 Mar 2012.) <http://www.centerbraininc.com/success/kimberly-clark.php> Moderate to severe incontinence actually affects as many as 3-17% of all women — although the older you are, the higher the incidence. For men it’s about half that at 3-11%. The severity of urinary incontinence ranges from occasionally leaking urine when you cough or sneeze to having an urge to urinate that’s so sudden and strong you don’t get to a toilet in time.14 Victor W Nitti. “The Prevalence of Urinary Incontinence.”Rev Urol. 2001; 3(Suppl 1): S2–S6. <http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1476070/> It can be caused by everyday habits, underlying medical conditions, or physical problems. And it can be temporary or chronic.
Temporary causes include:
- Certain medications such as heart medications, blood pressure drugs, sedatives, and muscle relaxants may contribute to bladder control problems.
- Alcohol acts as a bladder stimulant and a diuretic, which can cause an urgent need to urinate.
- Caffeine is a diuretic and a bladder stimulant that can cause a sudden need to urinate.
- Bladder irritation caused by certain foods or spices, including artificial sweeteners, citrus, and tomatoes — all of which can irritate your bladder.
- Heart meds, blood pressure drugs, sedatives, muscle relaxants, and other medications may contribute to bladder control problems.
Eliminating any of those causes will, in most cases, eliminate the problem. Other more systemic problems require more complicated solutions.
- Urinary tract infections can irritate your bladder, resulting in episodes of incontinence.
- The rectum is located near the bladder and shares many of the same nerves. Fecal matter stored in the rectum as the result of constipation can over-stimulate those nerves. Fecal matter backed up in the bowel can cause the bowel to press on the bladder, forcing out urine at inappropriate times. Excessive belly fat can have the same result — as can an enlarged uterus during pregnancy, or a prolapsed transverse colon.
- The stress of a vaginal delivery can weaken muscles needed for bladder control. The changes that occur during childbirth can also damage bladder nerves and supporting tissue, leading to a dropped (prolapsed) pelvic floor. With prolapse, your bladder, uterus, rectum, or small bowel can get pushed down from their usual position and protrude into the vagina. Such protrusions can be associated with incontinence.
- Aging of the bladder muscle can lead to a decrease in the bladder’s capacity to store urine and an increase in overactive bladder symptoms.
- Hormonal changes, particularly as the result of menopause can negatively affect the lining of the urethra and bladder, which can aggravate incontinence.
- In women, the bladder and uterus lie close to one another and are supported by many of the same muscles and ligaments. Any surgery that involves a woman’s reproductive system — a hysterectomy, for example– may damage the supporting pelvic floor muscles, which can lead to incontinence.
- In older men, incontinence often stems from enlargement of the prostate gland.
- Surgery or radiation used in treating prostate cancer can damage the nerves located near the prostate, which can affect bladder control.
The trick in treating incontinence is to identify the cause and eliminate the cause. For example, if the incontinence is the result of a urinary tract infection, getting rid of the infection will usually resolve the incontinence at the same time. Damage to nerves, however, is not so easy to repair.
 And finally, there are muscles involved in controlling urination. Like any muscles, without focused exercise, these muscles weaken over time. For most people, they never weaken so much that you have a problem, but if the weakening goes too far, you can become incontinent. There are ways to consciously exercise the muscles involved in urination, which will often help eliminate the incontinence if there isn’t a serious underlying problem such as a cancer. The standard exercise for controlling incontinence in both men and women is the Kegel (named after Dr. Arnold Kegel). The bottom line is that when it comes to the muscles involved in bladder control, the old exercise adage applies, “Use it or lose it.”
And finally, there are muscles involved in controlling urination. Like any muscles, without focused exercise, these muscles weaken over time. For most people, they never weaken so much that you have a problem, but if the weakening goes too far, you can become incontinent. There are ways to consciously exercise the muscles involved in urination, which will often help eliminate the incontinence if there isn’t a serious underlying problem such as a cancer. The standard exercise for controlling incontinence in both men and women is the Kegel (named after Dr. Arnold Kegel). The bottom line is that when it comes to the muscles involved in bladder control, the old exercise adage applies, “Use it or lose it.”
- Kegel exercise for women15 “Pelvic Floor (Kegel) Exercises for Urinary Incontinence in Women.” WebMD. (Accessed 5 Mar 2012.) <http://www.webmd.com/urinary-incontinence-oab/pelvic-floor-kegel-exercises-for-urinary-incontinence-in-women>
- Kegel exercise for men16 “Kegel Exercises: Treating Male Urinary Incontinence.” WebMD. (Accessed 5 Mar 2012.) <http://men.webmd.com/kegel-exercises-treating-male-urinary-incontinence>
When doing Kegels, you are likely to experience two surprises. First is how weak your muscles feel when you first try and isolate them. The second surprise is how quickly they strengthen if you exercise them for just a few minutes a day.
Next newsletter
In part 2 of our series on the urinary system, we’ll take a more detailed look at exactly:
- How the kidney’s filtration system works
- What can go wrong
- And how you can make things right again
References
| ↑1 | “Kidney and Urologic Diseases Statistics for the United States.” National Kidney & Urologic Diseases Information Clearinghouse (NKUDIC). (Accessed 3 Mar 2012.) <http://kidney.niddk.nih.gov/KUDiseases/pubs/kustats/index.aspx> |
|---|---|
| ↑2 | Pradeep Arora. “Chronic Kidney Disease.” Medscape Reference. Updated 16 Feb 2012. (Accessed 3 Mar 2012.) <http://emedicine.medscape.com/article/238798-overview#a0156> |
| ↑3 | “Kidney Stones in Adults.” National Kidney & Urologic Diseases Information Clearinghouse (NKUDIC). (Accessed 3 Mar 2012.) <http://kidney.niddk.nih.gov/kudiseases/pubs/stonesadults/> |
| ↑4 | Victoriano Romero, Haluk Akpinar, and Dean G Assimos. “Kidney Stones: A Global Picture of Prevalence, Incidence, and Associated Risk Factors.”Victoriano Romero, Haluk Akpinar, and Dean G Assimos. “Rev Urol. 2010 Spring-Summer; 12(2-3): e86–e96. <http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2931286/> |
| ↑5 | Sandra H. Berry, Marc N. Elliott, Marika Suttorp, Laura M. Bogart, et al. “Prevalence of Symptoms of Bladder Pain Syndrome/Interstitial Cystitis Among Adult Females in the United States.” I, v. 186, no. 2, Aug. 2011, p. 540-544. <http://download.journals.elsevierhealth.com/pdfs/journals/0022-5347/PIIS0022534711035452.pdf> |
| ↑6 | Clemens JQ, Meenan RT, Rosetti MC, Gao SY, Calhoun EA. “Prevalence and incidence of interstitial cystitis in a managed care population.” J Urol. 2005 Jan;173(1):98-102; discussion 102. <http://www.ncbi.nlm.nih.gov/pubmed/15592041> |
| ↑7 | Foxman B. “Epidemiology of urinary tract infections: incidence, morbidity, and economic costs.” Am J Med. 2002 Jul 8;113 Suppl 1A:5S-13S. <http://www.ncbi.nlm.nih.gov/pubmed/12113866> |
| ↑8 | “Vaginal Yeast Infections.” I. (Accessed 3 Mar 2012.) <http://www.obgynvirginia.com/conditions_And_Treatments/yeast-infections.php> |
| ↑9 | Buckley BS, Lapitan MC; Epidemiology Committee of the Fourth International Consultation on Incontinence, Paris, 2008. “Prevalence of urinary incontinence in men, women, and children–current evidence: findings of the Fourth International Consultation on Incontinence.” I. 2010 Aug;76(2):265-70. Epub 2010 Jun 11. <http://www.ncbi.nlm.nih.gov/pubmed/20541241> |
| ↑10 | Avorn J, Monane M, Gurwitz JH, Glynn RJ, Choodnovskiy I, Lipsitz LA. “Reduction of bacteriuria and pyuria after ingestion of cranberry juice.” JAMA 1994;271:751-754. <http://jama.ama-assn.org/content/271/10/751.abstract> |
| ↑11 | Zafriri D, Ofek I, Adar R, Pocino M, Sharon N. “Inhibitory activity of cranberry juice on adherence of type 1 and type P fimbriated Escherichia coli to eucaryotic cells.” Antimicrob Agents Chemother 1989;33:92-98. <http://www.ncbi.nlm.nih.gov/pmc/articles/PMC171427/> |
| ↑12 | Ofek I, Goldhar J, Zafriri D, Lis H, Adar R, Sharon N. “Anti-Escherichia coli adhesin activity of cranberry and blueberry juices.” N Engl J Med 1991;324:1599-1599. <http://www.nejm.org/doi/full/10.1056/NEJM199105303242214> |
| ↑13 | “Kimberly-Clark – Depend Protective Underwear.” Centerbrain. (Accessed 6 Mar 2012.) <http://www.centerbraininc.com/success/kimberly-clark.php> |
| ↑14 | Victor W Nitti. “The Prevalence of Urinary Incontinence.”Rev Urol. 2001; 3(Suppl 1): S2–S6. <http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1476070/> |
| ↑15 | “Pelvic Floor (Kegel) Exercises for Urinary Incontinence in Women.” WebMD. (Accessed 5 Mar 2012.) <http://www.webmd.com/urinary-incontinence-oab/pelvic-floor-kegel-exercises-for-urinary-incontinence-in-women> |
| ↑16 | “Kegel Exercises: Treating Male Urinary Incontinence.” WebMD. (Accessed 5 Mar 2012.) <http://men.webmd.com/kegel-exercises-treating-male-urinary-incontinence> |







Jon – sure hope there is a
Jon – sure hope there is a part three that continues on to the
prostate ! LOL
Would love to see the kind of info you put out on THAT subject !
Although it affects
Although it affects urination, the prostate is actually part of the reproductive system — unless you're urinating in an unusual manner.
I have an enlarged prostate.
I have an enlarged prostate. Hard to pee and no ejaculate? Any help? Thanks
Thank You!! This is great
Thank You!! This is great information.
Greg
Thanks, Jon, for another
Thanks, Jon, for another superb article. Your in-depth research and clarity of expression make for an enjoyable and useful learning experience for your visitors.
Would like to receive Kegel
Would like to receive Kegel exersizes
Armin, You don't "receive"
Armin, You don't "receive" Kegel exercises, you DO them! If you look at the article again, it shows a link on Kegel exercises for men. It will show you how to do them. I'm a woman and I do the Kegel exercises for women and it has helped my bladder problems a lot, so I hope you find help for whatever you need.
LOts of great information!
LOts of great information!
Jon,
You always have such
Jon,
You always have such informative topics. I enjoy them all. Thank You!
This is the most informative
This is the most informative print on the kidneys and urinary system I’ve read in a long time. Also, more easily understood! Thanks!
THANKS AGAIN JON. AS USUAL,
THANKS AGAIN JON. AS USUAL, INFORMATIVE AND HELPFUL.
This is a good common sense
This is a good common sense Blog. Very helpful to one who is just finding the resources about this part. It will certainly help educate me.
Very impressive and
Very impressive and informative!