In Part 1 of our series on the digestive system, we explored the process whereby food enters the stomach through the mouth and esophagus. We now pick up the process as the food arrives in the stomach.
In the introduction portion of our series on the digestive system called “Overview of the Digestive System,” we overviewed the process whereby food enters the mouth and passes through the GI tract and on out through the anus. We also focused on the process of actually getting food into the stomach through the mouth and esophagus. And finally, we discussed how enzymatic digestion begins in the mouth, but for most people, because of diet and eating habits, never actually amounts to much.
We now pick up the process as the bolus of food arrives in the cardia of the stomach — which brings us to our first key point of the day that although the stomach has no actual physical separations, it does not function as an undifferentiated sac.
The divisions of the stomach
Anatomically, the stomach is not so much a separate organ as it is an enlargement (like the esophagus) of the intestinal tract that sits just below the diaphragm. In fact, the only thing that separates it from the rest of the GI tract are areas at its top and bottom that use muscles to constrict and close it off from the esophagus and the duodenum on either end respectively. Its functions are very simple: to grind, mix, digest, and parcel out its contents to the intestinal tract in a slow, controlled manner.
Although it is a single cavity (again, just part of the GI tract), it has four main “functional” divisions. Physiologically speaking, they are:
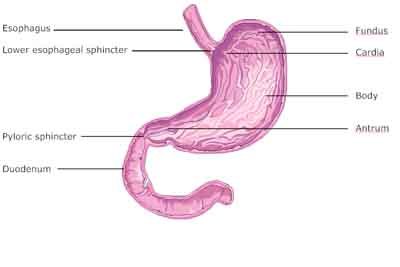
- The cardia, which is a small space at the very entrance to the stomach that sits just under the diaphragm and the heart. In fact, the cardia is named for its proximity to the heart. It is the landing area for the bolus (clump of chewed food) that you swallow and that drops down from the esophagus. Note: once the stomach starts working on the bolus, grinding it down and mixing it with enzymes and acids, it acquires a new name. This semi-digested glop (a non-medical term) is called chyme. You would be familiar with chyme if you’ve ever vomited.
- The fundus, which is the main upper portion of the stomach. Fundus means “enlargement” and refers to the rounded enlarged area at the top of the stomach. Food gets ground, mixed, and held in the fundus. It is in the fundus that enzymatic digestion takes place, assuming there are live enzymes present with your meals (or if you are using digestive enzyme supplements). Although stomach acid will be released into the fundus, it is only at about 30% concentration and will not affect enzymatic digestion. After about 40-60 minutes in the fundus, the chyme will move on into the body of the stomach.
- The body, which is the large middle section of the stomach. It is a primary area of digestion, and it is here that hydrochloric acid and pepsin begin to work full bore, and at levels sufficient to stop most enzymatic digestion.
- The antrum, which is the last part of the stomach before the pylorus, the gate which prevents food from entering the intestine before its time. Actually, the major portion of digestion takes place in the antrum as food is held a long time and parceled out to the duodenum in a very slow, methodical manner. Incidentally, antrum means cave and pylorus means gatekeeper.
The chyme moves through these divisions sequentially, rather than just dumping into one great cavity. This distinction is crucial to understanding the digestive process. Unfortunately, although medical doctors understand the sequential nature of digestion in the stomach, they do not fully understand what it means. And once again, that’s because they base their assumptions on observation; and when it comes to observation, 99.9% of the people they see eat the typical highly processed, cooked food “modern” diet — not the more natural diet our bodies were designed to handle. In other words, doctors’ assumptions about digestion are based on observing people who eat badly, consume food totally devoid of live enzymes, and gulp their food down so quickly it barely has any time to mix with salivary enzymes. This gives a very distorted view of how the digestive process “should” work. And it has profound implications for our understanding of the digestive process and the things that can go wrong with it — all of which, we will talk more about later.
For now, just understand that food moves through the divisions of the stomach sequentially. Among other things, this allows us to consume more than the intestines are ready for at one time. The divisions allow us to process the food slowly and prepare it for entry into the intestines in a controlled and measured manner.
 The layers of the stomach
The layers of the stomach
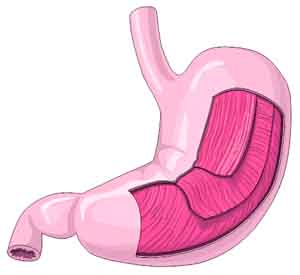
The outer covering of the stomach is called the serosa. Its primary purpose is to carry blood vessels and to protect the stomach. The stomach is supplied by an extremely rich supply of blood vessels. Just under the serosa are the layers of muscle — longitudinal, circular, and oblique.
As you can see from the illustration to the right, these muscles allow the stomach to bend, twist, and fold in almost any direction. Combine all of that motion with the folds (rugae) in the interior of the stomach (as shown in our previous illustration of the stomach’s divisions) and it’s easy to see how the stomach can easily “grind” food down and totally mix it up with any digestive enzymes and juices that are present.
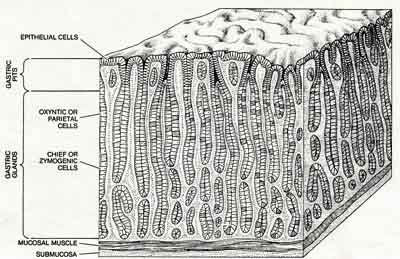
One final layer that we need to talk about is the thick, plush layer of mucosa cells that line the stomach cavity. It has deep clefts that increase the stomach’s surface area considerably. There are four different types of mucosa cells.
- Epithelial cells cover the surface of the stomach and also line the gastric pits. Specifically, mucosal neck cells are the most numerous cells in the stomach. They function as glands and produce a thick glycoprotein (sugar and protein together) mucous that is greasy to the touch and coats everything it touches. It protects the stomach wall from autodigestion by keeping the stomach juices from actually touching any tissue and digesting the stomach (most of the time). Any defects in the glycoprotein covering will lead to erosions, ulcers, and even autodigestion of the stomach wall.
- Parietal cells produce stomach acid (HCL) and intrinsic factor, which helps absorb vitamin B-12. They are located only in the fundus and body of the stomach. Along with “chief cells,” these cells lie in deep tubules; their secretions reach the surface through “gastric pits.” (see illustration)
- Chief cells produce pepsinogen (the precursor to pepsin) and gastric lipase (a fat-digesting enzyme).
- And finally, there are the enteroendocrine cells (G-cells) located in the antrum that produce the hormone gastrin. Gastrin is secreted directly into the bloodstream and makes its way back to the fundus and body of the stomach to stimulate parietal cells to produce more hydrochloric acid. (Hormones are signalers.) The triggers for gastrin production are the physical distension of the antrum (as “too much” food presses its way in) and any rise in pH, which signals receptors in the antrum that the acid levels of the chyme have become too diluted.
Digestion
There are two main kinds of digestion processes in the stomach:
- Mechanical
- Chemical
Mechanical digestion is defined by the stomach’s mixing of the chyme, whereas chemical digestion is defined by the action of various acids, hormones, and enzymes on the chyme.
Mechanical digestion
After the bolus drops into the cardia, it is pushed up into the fundus, where it is held for upwards of 40-60 minutes with minimal stomach acid being produced — about 30% of full levels and not enough to render digestive enzymes inactive. It is while in the fundus that enzymatic digestion (from live enzymes present in the food, salivary enzymes introduced while chewing, or supplemental digestive enzymes taken with your meal) takes place. Up to 75% of digestion can take place during this phase — or none at all if there are no enzymes present. Since any sustained heat of approximately 118-129 degrees F destroys virtually all enzymes, it’s easy to see why the modern diet is pretty much devoid of live enzymes. Add to this the fact that the vast majority of people don’t really chew their food but, rather, gulp it down — thus missing out on salivary enzymes as well — and you have the very real potential for zero enzymatic digestion taking place in the fundus.
Once again, enzymatic digestion is almost never accounted for in medical texts because doctors rarely see it. Again, ninety-nine percent of their patients eat cooked/processed food that is devoid of digestive enzymes and chew their food minimally so there is very little salivary action on the food. In any case, when doctors look at the cardia and fundus, they primarily see holding areas where virtually no enzymatic digestion takes place.
One nod the medical texts do give to the fundus is that it’s where ghrelin is manufactured. Ghrelin is a hormone produced mainly by the P/D1 cells lining the fundus. The key role ghrelin plays is that it stimulates hunger. It is considered the counterpart of the hormone leptin, produced by fatty tissue, which induces satiation when present at higher levels.
In any case, at the end of “fundal” cycle, whether any enzymatic digestion has taken place or not, the chyme is moved down into the body of the stomach, where stomach acid is introduced at full levels, thus neutralizing all enzyme activity. Very little mixing takes place in the cardia or the fundus (again, these areas are reserved primarily for enzymatic digestion) but commences full force once the chyme is in the body of the stomach. In fact, waves of peristalsis (muscle contractions) grind and mix the food once in the body. This action is aided by the rugae, or folds, in the interior of the stomach, which force the chyme to roll over and churn as the muscular contractions squeeze the chyme over the folds.
After a period of intense mixing and digestion, the chyme moves from the body of the stomach into the antrum, where it is held up. The body knows that the duodenum is very small. Therefore, only a small amount of chyme is allowed into the duodenum at any given time; the rest remains in the antrum for additional mixing and grinding and additional chemical digestion. In fact, the major chemical processes take place, not in the body of the stomach, but in the antrum while chyme is waiting its turn to pass through the pyloric valve.
And with that stated, now let us take a closer look at these chemical processes.
Chemical digestion
When we refer to chemical digestion, we’re talking about the action of hydrochloric acid and pepsin (or parietal cells and chief cells) on the chyme. At its most basic level, chemical digestion is about taking big molecules and breaking them down into smaller molecules. Note: enteroendocrine cells are also active in the stomach, but (as we will discuss later) they play a regulatory role, rather than a digestive role. Let us now look at the different cells in the stomach that play the major roles in chemical digestion.
Parietal cells
There are some parietal cells in the fundus, but most are in the body of the stomach and the antrum. The parietal cells are extremely important as they secrete hydrochloric acid (HCL) in very high concentrations.
HCL performs the following functions.
- It denatures (unfolds) proteinsso that they can actually be broken down by pepsin during digestion. Without being unfolded, they resist digestion. Understand, proteins are chains of amino acids that are folded in on themselves — and can only function when they are geometrically correct in these folds. Denaturing means they are made inactive in the physiological sense by breaking the bonds that hold their geometric shape and allowing the proteins to unfold into long chains — which can then be broken apart into component amino acids. It should be noted that denaturing proteins can have two entirely different effects depending on how complete the denaturing is; and if not complete, what variation of the protein is left. A major factor in determining that outcome is how the denaturing is accomplished (heat VS acid) and on which protein it is effected (e.g., meat VS dairy).
- As a rule of thumb, acid denaturing as takes place in the stomach is beneficial and assists in the digestion of the protein.
- Denaturing as caused by heat applied to food before digestion takes place can often produce versions of a particular protein that are highly indigestible and highly allergenic. This is the primary reason that pasteurized dairy is so much more allergenic than raw dairy.
- HCL kills many micro-organisms, such as the ones that travel into the digestive tract from the human mouth or come breeding in the food itself — as with contaminated meat or produce. (Note: the human mouth is so dirty, you’d rather be bitten by a dog than another person.)
- HCL stimulates the flow of hormones, bile juices, and pancreatic juices in preparation for release into the small intestine. In other words, it is a key trigger for all aspects of the digestive process. Note: this is where live food makes a difference. The more enzymatic digestion that takes place before this point, the less HCL is required to finish the process. The less HCL produced, the less pancreatic juices are signaled for — thus sparing the pancreas a great deal of work.
- HCL inhibits the activity of the hormone gastrin in a negative feedback loop. We will talk more later about how gastrin is released into the bloodstream and stimulates the flow of HCL. But, for now, as HCL builds up, the increase in HCL signals that less gastrin be produced — thus leading to the lessening and stopping of HCL production. This makes perfect sense as it’s a simple way for the body to prevent over production of stomach acid. Unfortunately, this loop is easily disrupted. This fact will become particularly important when we talk about antacids such as Tums and proton pump inhibitors such as Prilosec, Prevacid, and Nexium a little later.
- And finally, when the chyme passes into the duodenum, the HCL stimulates the release of secretin (which regulates pH in the intestinal tract) and cholecystokinin (CCK), which regulates the flow of bile and pancreatic enzymes and prepares the small intestine for the chyme headed its way. And here again we can see a primary problem with not having sufficient enzymatic digestion take place higher up in the stomach. The less digestion that takes place in the cardia and fundus, the more acid will be required to make up the difference in the body of the stomach and the antrum. The higher the levels of HCL in the chyme that passes into the duodenum, the higher the levels of CCK that will be called forth. And the higher the levels of CCK called forth, the more pancreatic enzymes your body will be forced to produce in anticipation of what’s coming down the chute and the more bile your liver will have to produce to compensate. This is the reason virtually everyone consuming a modern diet has an enlarged pancreas by the time they are 40. In fact, it is so common that an asymptomatic enlarged pancreas is now considered “normal” as people age. Normal???
Chief cells
Pepsinogen is secreted by the chief cells. By itself, pepsinogen is inactive and will digest nothing until it is converted into pepsin when it comes in contact with the hydrochloric acid in the stomach. Pepsin is an extremely powerful protein digestive enzyme that thrives in a high acid environment. Pepsinogen converts to active pepsin only at low (high acid) pH. This is actually a remarkably elegant maneuver by your digestive system. Since pepsin literally digests protein, you don’t want pepsin active in the mucosal/chief cells or it would digest them. Thus the mucosal cells release pepsinogen, pepsin’s precursor — which is converted into pepsin only after the pepsinogen has made its way out of the chief cells and into the stomach itself, where it is converted in the presence of stomach acid. Since the wall of the stomach is coated with a glycoprotein mucous, the pepsin can only digest your meal and not your stomach.
As we discussed already, stomach acid doesn’t actually digest protein; it merely unfolds the proteins. That’s where pepsin comes in. Pepsin is what actually breaks bonds between amino acids that make up proteins; thus, it is the pepsin that literally digests proteins. (Actually, it breaks them into “peptides,” which are smaller chains of amino acids.) And once again, if your body is getting the benefit of full enzymatic digestion in the cardia and fundus, it will digest up to 75% of the proteins in your meal before HCL and pepsin ever come into play. This means that in proper digestion, HCL and pepsin should only be required to do clean up duty. But without enzymatic digestion, your body is required to increase HCL and pepsinogen production by some 400% to make up the difference. Once again, this is a major body stressor with profound long term consequences.
Pepsinogen serves one other key function in the stomach: it plays a significant role in moving chyme through the digestive tract. Or in “medicalese,” it increases gastric motility. It accomplishes this in two ways. First, it is the arrival of pepsinogen that plays a key role in telling the esophageal sphincter to close down so that food and stomach acid can’t back up into the esophagus. Pepsinogen then works at the other end of the stomach by telling the pyloric sphincter to open, thus allowing food to exit the stomach and make its way into the duodenum.
The chief cells also secrete gastric lipase, which breaks triglycerides into fatty acids and monoglycerides. Unlike triglycerides, fatty acids and monoglycerides are usable by your body and do not promote heart disease. It should also be noted that because gastric lipase is active at a pH of 3-6, its role is somewhat limited until it enters the duodenum, where stomach acid is neutralized and pH is raised. Another note is that although salivary lipase and gastric lipase are overshadowed by the later action of pancreatic lipase in the intestinal tract, if allowed to do their job, the action of salivary and gastric lipase can significantly reduce the burden of pancreatic lipase in the intestinal tract. Once again, we pay a price for our modern diets — unless we supplement with digestive enzymes.
Enteroendocrine cells
Enteroendocrine cells, which are also known as G-cells, are located primarily in the antrum and release gastrin which stimulates the production of both HCL and pepsinogen in the antrum and higher up in the body of the stomach. It is able to signal higher up in the stomach because the gastrin is released into the bloodstream and circulates around until it can enter the blood vessels that feed the stomach all the way from the esophageal sphincter to the pyloric valve. In addition to promoting digestive juices, gastrin causes the lower esophageal sphincter to relax; thus, high levels of gastrin are thought to play a role in the development of acid reflux disease since they cause the valve to relax too much and at inappropriate times. This will become significant when we talk about using antacids and proton pump inhibitors since by dramatically lowering HCL levels during digestion they cause a concomitant jump in gastrin levels in an attempt to ramp HCL levels back up. The net effect is a much “looser” esophageal valve thus allowing chyme to back up into the esophagus more easily. Taking this into consideration, high levels of gastrin may play a significant role in the development of acid reflux disease.
It probably should be mentioned that G-cells produce these higher levels of gastrin in response to antacids and proton inhibitors by proliferating wildly so that there are more of them to produce gastrin. So once again, artificially forcing symptoms back in line with pharmaceutical drugs has consequences. Although, to be fair, there is no evidence yet that this proliferation of cells leads to a malignant transformation in patients using the drugs. Then again, is that a risk you want to take?
Conclusion
In our discussion of the stomach so far, we have learned exactly how the lack of enzymes in our food affects digestion and why supplementation with a good digestive enzyme formula makes sense. We have also picked up strong indications as to why antacids and proton pump inhibitor drugs may not be the best long term solutions to acid reflux. In fact, you may never look at your stomach in the same way again.
In our next issue, we will conclude our discussion of the anatomy and physiology of the stomach, as we:
- Examine the three phases of gastric secretion
- Take a look at the duodenum
- Explore how the stomach empties itself
- Return to our discussion from the last newsletter on the difference between the digestive tracts of carnivores, omnivores and frugivores
And finally, we’ll finish with the big payoff on our discussion of the stomach with an examination of the things that can go wrong and how to prevent and even cure them, such as:
 Acid reflux
Acid reflux- Peptic ulcers
- Problems with mineral absorption
- Inadequate B12 absorption
- The aging stomach
- Things that contribute to incomplete digestion
- Satiety VS overeating
Continue reading Jon’s series about digestive health:
Overview of the Digestive System
Your Stomach, Part 2
Your Stomach, Part 3







ABOVE, IT IS STATED PART 1
ABOVE, IT IS STATED PART 1 WAS REVIEWED (PAST TENSE?)
BUT THE ABOVE IS PART 1!! SHOULDN’T IT BE STATED THAT PART 1 WILL BE DISCUSSING …… ? I DON’T GET IT!!
Dr. Robert Bolmarcich
PH.D M.E.
Sorry, he meant: “Overview
Sorry, he meant: “Overview of the Digestive System“. You are correct, this article is Part 1. We updated the top for clarity.