
Introduction and getting food into the digestive tract
In this issue, we begin a series on the digestive system. Effectively, this system is a continuous tube from the mouth to the anus — something you probably don’t want to think about the next time you kiss someone. Over the course of the next half dozen or so newsletters, I’m going to walk you through the digestive system — from the tip of your tongue to the outer edge of your rectum. We’re going to cover the anatomy and physiology of everything from your teeth to your bowel, plus the organs of digestion including the liver, gallbladder, and pancreas. All of this will help you understand the nature of diseases of the digestive tract (everything from hiatal hernia to acid reflux, from peptic ulcers to irritable bowel syndrome) and how to treat them naturally by working with your body, not against it.
Along the way, I’m going to be challenging a number of medical assumptions. How can that be? Aren’t anatomy and physiology pretty much cut and dried? And the answer is: “Not necessarily.” As it turns out, the body responds differently according to what you eat, how you eat it, and how that food is prepared. Virtually, all physiological assumptions used by the medical community are based on observation of people eating the typical high speed modern diet. Change the diet, and you change the physiology.
And in fact, these differences are critical. It has been said that we dig our graves one forkful at a time. By understanding exactly how our body processes what we eat and how what we eat affects those processes, we can change our health outcomes. Effectively, we can delay the digging of our graves for years. And maybe even more importantly, we can enjoy those years with a much higher level of health and vitality. I’m sorry, but people who tell me they are perfectly healthy because they are successfully “managing” their acid reflux and Crohn’s disease with medications are not actually healthy. They are merely suppressing the symptoms of unhealth…temporarily.
Obviously, this is a huge topic and can’t be covered in one newsletter. Effectively, I’m going to break the discussion into several pieces, including:
- Getting food into the digestive tract — the mouth and esophagus
- The organs that support digestion — the liver, gallbladder, and pancreas
- Absorbing nutrients — the small intestine
- Processing and eliminating the waste — the colon
Digestive system overview
Before we launch into the focus of today’s newsletter, the mouth and esophagus, let’s take a quick overview of the entire system.
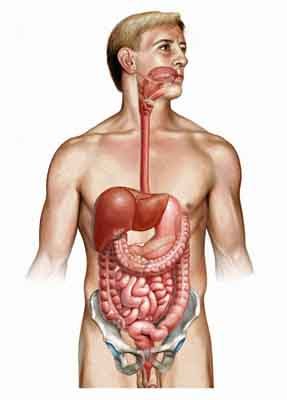 The digestive system is also known as the gastrointestinal (GI) tract and the alimentary canal and covers everything from the digestive tract itself to the organs that support it. It is a continuous tube-like structure that develops outpouchings, which in turn evolve into those aforementioned attached digestive organs such as the pancreas, liver, and gallbladder. The entire system is about 30 feet in length from the mouth to the anus and is designed to transport food and water, modify it, and make it suitable for absorption and excretion. There are storage sites, excretion sites, and detoxifying sites along the way. And, according to the medical community, it has six primary functions.
The digestive system is also known as the gastrointestinal (GI) tract and the alimentary canal and covers everything from the digestive tract itself to the organs that support it. It is a continuous tube-like structure that develops outpouchings, which in turn evolve into those aforementioned attached digestive organs such as the pancreas, liver, and gallbladder. The entire system is about 30 feet in length from the mouth to the anus and is designed to transport food and water, modify it, and make it suitable for absorption and excretion. There are storage sites, excretion sites, and detoxifying sites along the way. And, according to the medical community, it has six primary functions.
- Ingesting food.
- Preparing food for digestion by physically grinding it and breaking it down into small pieces and unwinding proteins so they can be separated into their component amino acids.
- Actually breaking the food into molecular pieces that your body can use as nourishment.
- Transporting the food during its various stages of breakdown along the digestive tract in a measured, “manageable” flow.
- Absorbing the nutrients into the body. Absorption is the movement of broken-down nutrients across the digestive tract wall and into the bloodstream for use by the cells of the body. Only water and alcohol are absorbed through the mucosa of the stomach – and only in special circumstances such as severe dehydration. All the rest of absorption happens in the small intestine.
- Eliminating the unused waste products of digestion and absorption from the body.
- Digested waste products go to the kidneys
- Undigested waste products pass out through the colon and rectum.
- Ingested material that might otherwise be toxic is rendered harmless, primarily by the liver, and excreted from the body.
But that said, I now have my first disagreement with the medical community. I submit to you that the above list is incomplete, and that these omissions are not unimportant. For example, medicine has no understanding of the role your digestive system plays in maintaining an optimal environment for beneficial bacteria and why that’s essential. Therefore, they both allow and, in fact, encourage by their treatments many diseases to manifest that should never appear — and have no idea how to treat them when they do. And that’s just one example that we’ll explore in more detail later on. So, from a holistic point of view, the digestive system, in addition to the functions listed above, also performs the following functions:
- It is the first line of defense in the body’s immune system. It both identifies and eliminates viruses and unhealthy bacteria ingested with our food and water.
- It plays a key role in helping remove, not just food waste from the body, but also metabolic waste, heavy metals, and drug residues.
- It also serves as a drain for toxic substances absorbed through the skin and lungs.
- And, of course, as mentioned above, it is designed to serve as a hospitable breeding ground for trillions of beneficial bacteria that do everything from aiding in digestion, waste elimination, and immune function. In fact, as much of 60% of your immune function comes from beneficial bacteria living in your intestinal tract.
Carnivore, omnivore, frugivore?
 There is one other piece of overview information we need to cover. The medical community bases its assumptions concerning the human digestive system on the “fact” that it is essentially designed as an omnivore system. (Only people at tailgate parties and gladiator games actually believe that we are pure carnivores.) But, as I discussed in detail in Lessons from the Miracle Doctors, this is simply not supported by the evidence at hand. And once again, this distinction is not subtle…and not insignificant. Yes, the human body has an amazing ability to adapt to any diet we throw at it — but not without consequences. And, in fact, many of the diseases we face today are the direct result of not understanding what our systems are designed to handle and the consequences we face as a result.
There is one other piece of overview information we need to cover. The medical community bases its assumptions concerning the human digestive system on the “fact” that it is essentially designed as an omnivore system. (Only people at tailgate parties and gladiator games actually believe that we are pure carnivores.) But, as I discussed in detail in Lessons from the Miracle Doctors, this is simply not supported by the evidence at hand. And once again, this distinction is not subtle…and not insignificant. Yes, the human body has an amazing ability to adapt to any diet we throw at it — but not without consequences. And, in fact, many of the diseases we face today are the direct result of not understanding what our systems are designed to handle and the consequences we face as a result.
How could the medical community be so wrong on this issue? Actually, it’s very simple, and it’s the same old problem. As usual, the medical community views the body as separate pieces, not as an integrated whole. It looks at things in isolation. In this particular case it looks at the diet of the 99% of population that passes through their doors in need of their care, and those people eat everything from cotton candy to slabs of grilled beef — an omnivore diet. Given this context, for medical anatomists, the digestive system is undeniably designed for an omnivore diet. However, it takes only a slightly more holistic viewpoint to make a casual comparison of the structures of the human digestive system (teeth, stomach, and intestines) to other animals living in the wild to see how unsupportable that point of view is. And in fact, we will cover those differences in detail as we move through the digestive system and discuss each relevant organ.
And with all that said, let’s now begin our trip through the digestive system.
Getting food into the digestive tract — the mouth and esophagus
Let’s begin our exploration of the digestive system by examining the structures that play a key role in getting the food into the stomach. And since this is not an actual anatomy course, but a series of newsletters about how anatomy and physiology relate to alternative health, we will focus our discussion on the specific parts of the system relevant to our discussion and brush lightly over the rest.
Mouth
The mouth is the portal to the digestive system. Food enters the body through the mouth, where it is cut and ground by the teeth and moistened by saliva for ease in swallowing and to start the digestive process. The tongue assists in moving food around during chewing and swallowing and also contains the taste buds.
Teeth
Most medical texts suggest that our teeth are designed to eat all kinds of food from meat to fruit, thus proving that man is an omnivore. But as I mentioned earlier, the facts do not bear this out. Here is a human skull and teeth.

Notice how all of the teeth are nearly the same height. Our canines project only a small amount, and our molars are broad-topped.
 Compare this to the teeth of a carnivore such as lion.
Compare this to the teeth of a carnivore such as lion.
The first thing you notice about carnivores is that their teeth are nothing like those found in humans. They have huge canines for striking and seizing prey, pointed incisors for removing meat from bones, and molars and premolars with cusps for shredding muscle fiber. In carnivores, the teeth of the upper jaw slide past the outside of the lower jaw so that prey is caught in a vice-like grip. In general, carnivores don’t chew much; mostly, they just tear chunks off and swallow them whole. All in all, nothing like human teeth.
 But the claim in medical texts is that we are omnivores, not carnivores. How does that claim stand up? Well, first of all, no animal is really adapted to eat all things, but if any animal comes close, it would be the bear. Typical foods consumed by bears include ants, bees, seeds, roots, nuts, berries, insect larvae such as grubs, and even flowers. Some meat, of course, is eaten by bears, including rodents, fish, deer, pigs, and lambs. Grizzlies and Alaskan brown bears are well-known salmon eaters. Polar bears feed almost exclusively on seals, but then, what vegetation is there for them to eat in the frozen wastes of the Arctic? And, of course, anyone who has read Winnie the Pooh knows that many bears love honey. So, other than the ants, grubs, and rodents, the bear diet sounds a lot like the typical Western diet. So let’s take a look at the bear’s teeth.
But the claim in medical texts is that we are omnivores, not carnivores. How does that claim stand up? Well, first of all, no animal is really adapted to eat all things, but if any animal comes close, it would be the bear. Typical foods consumed by bears include ants, bees, seeds, roots, nuts, berries, insect larvae such as grubs, and even flowers. Some meat, of course, is eaten by bears, including rodents, fish, deer, pigs, and lambs. Grizzlies and Alaskan brown bears are well-known salmon eaters. Polar bears feed almost exclusively on seals, but then, what vegetation is there for them to eat in the frozen wastes of the Arctic? And, of course, anyone who has read Winnie the Pooh knows that many bears love honey. So, other than the ants, grubs, and rodents, the bear diet sounds a lot like the typical Western diet. So let’s take a look at the bear’s teeth.
Notice, the bear has the sharp canines of the carnivore and the pronounced incisors of the herbivore. They also have molars that are both pointed and broad topped. That’s not even close to the human set of teeth pictured earlier.
 So, does that mean we are restricted to a diet of fruits and nuts? Not at all! In fact, the frugivores we most closely resemble, the wild chimpanzees, periodically eat live insects and raw meat. Notice the picture of a chimp’s teeth.
So, does that mean we are restricted to a diet of fruits and nuts? Not at all! In fact, the frugivores we most closely resemble, the wild chimpanzees, periodically eat live insects and raw meat. Notice the picture of a chimp’s teeth.
Other than the long canines, they are virtually identical to human teeth.
Among the great apes (the gorilla, the orangutan, the bonobo, and the chimpanzee) and ourselves, only humans and chimpanzees hunt and eat meat on a frequent basis. Gorillas have never been observed hunting or feeding on any animals other than invertebrates such as termites and ants. Nevertheless, chimpanzees are largely fruit eaters, and meat comprises only about 3 percent of their diet — far less than is found in the typical Western diet.
Bottom line: at least as defined by our teeth, we do not qualify as carnivores or omnivores. So, at least as judged by our teeth, meat should comprise no more than 3% of our diet. But teeth do not comprise the end of the issues. Later on, we’ll compare stomachs and intestinal tracts to see if we match up any better there.
Tongue
The tongue is the largest muscle in the mouth. It functions in chewing, swallowing, and forming words. The extrinsic muscles of the tongue (those muscles that originate outside the tongue itself) attach to the skull and neck, and they move from side to side and in and out. The intrinsic muscles attach to the tongue itself, and they alter the tongue’s shape (for swallowing and speech). The most interesting parts of the tongue in terms of our discussion are the papillae, the bumps on the tongue that contain the taste buds.
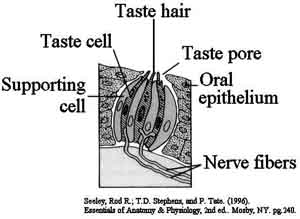 Taste buds are composed of groups of about 40 column shaped epithelial cells bundled together along their long axes. Taste cells within a bud are arranged such that their tips form a small taste pore. Minute, hair-like threads called microvilli extend through this pore from the actual taste cells. The microvilli of the taste cells bear the actual taste receptors, and it appears that most taste buds contain cells that bear receptors for two or three of the basic tastes.
Taste buds are composed of groups of about 40 column shaped epithelial cells bundled together along their long axes. Taste cells within a bud are arranged such that their tips form a small taste pore. Minute, hair-like threads called microvilli extend through this pore from the actual taste cells. The microvilli of the taste cells bear the actual taste receptors, and it appears that most taste buds contain cells that bear receptors for two or three of the basic tastes.
There are four tastes we normally associate with taste buds: sweet, salty, sour, and bitter. However, research has identified a fifth taste our buds can identify. The fifth taste is umami, the taste of monosodium glutamate (no kidding), and has recently been recognized as a unique taste, as it cannot be elicited by any combination of the other four taste types. Glutamate is present in a variety of protein-rich foods, and particularly abundant in aged cheese.
Unless artificially disrupted, our sense of taste will guide us to the foods necessary for our survival. And, in fact, our taste preferences change according to our body’s needs. Just ask the husband of any pregnant woman. Or more scientifically:
- Removal of the adrenal glands without replacement of mineralocorticoids leads rapidly to death due to massive loss of sodium from the body. Adrenalectomized animals (animals whose adrenal glands have been surgically removed) show a clear preference for salty water over pure water, and if provided with salt water, can actually survive.
- If the parathyroid glands are removed, animals lose calcium and cannot maintain blood calcium levels appropriately due to deficiency in parathyroid hormone. Following parathyroidectomy (removal of the parathyroid glands), animals choose drinking water that contains calcium chloride over pure water or water containing equivalent concentrations of sodium chloride.
- Injection of excessive doses of insulin results in hypoglycemia (low blood sugar). Following such treatment, animals will preferentially pick out and consume the sweetest among a group of foods.
Now, there are three tastes I want to focus on.
Sweet
The sweet taste was designed to cause us to desire natural carbohydrates essential for our survival. As we discussed above, our teeth match those of the frugivores, largely fruit eaters. However, technology has allowed food manufacturers to exploit our desire for sweet things — to our detriment. For the most part, concentrated sugars, other than honey, are not naturally available for us to consume. Table sugar is a manufactured creation, as is maple syrup, agave syrup, not to mention high fructose corn syrup, glucose, dextrose and all of the other concentrated sweeteners added to our food. If living in nature, our desire for sweets would lead us to low concentrations of sugar bound to fiber, not 32 oz Big Gulp sodas containing almost a cup of concentrated sugar. The bottom line is that these concentrated sweeteners feed an addiction because, based on evolution, our taste buds never expected to find concentrated sweeteners — only natural foods, with a far less concentrated character. And to make matters even worse, the more concentrated sweeteners we eat, the more we crave.
Umami
A similar situation exists with umami, also known as “savory.” In nature, this taste is never concentrated, and exists only in very small amounts in selected foods. Concentrating it as a food additive, confuses the system and allows us to consume glutamate in far higher levels than our bodies were ever designed to handle — with highly disruptive health effects for sensitive people.
Bitter
And then there’s bitter! Bitterness is the most sensitive of the five tastes. It has been suggested that the evolutionary purpose of “bitter” is to warn us against ingesting toxic substances, many of which have a bitter character. Unfortunately, this association between bitter and unhealthy is not entirely true, and our current culinary desire to avoid bitter tastes causes us to miss the health benefits associated with many bitters. Common bitter foods and beverages include coffee, unsweetened chocolate, bitter melon, beer, bitters, olives, citrus peel. But how many people eat them in their unadulterated form any more. Bitters are almost always masked by added sugar. In any case, whereas at one time people regularly consumed bitters as part of their diet, we pretty much completely avoid them now. When’s the last time you saw a fast food or soda pop based on bitter?
This has major health consequences for your liver. The body has a number of built-in feedback loops, a number of which we’ll cover as we move through the digestive system, such as the triggers that both stimulate and shut off the production of stomach acid. But the simple fact is that the taste of bitter in the mouth is stimulating to the liver. There is a direct feedback loop from the tongue to the liver. Every time you taste something bitter, your liver gets a positive jolt that stimulates it to put out more essential bio-chemicals and expel accumulated toxic waste. If you never taste any bitter, your liver tends to become sluggish over time and retain toxic build-up. This is one of the key reasons that the Liver Tincture and Blood Support™ formulas I use during detoxing have such a pronounced bitter taste. In fact, all of the great liver herbs, milk thistle, dandelion root, and Picrorhiza Kurroa are decidedly bitter.
Nose/Smell
Although not usually considered, anatomically, as part of the digestive system, the nose really does qualify. After all, up to 75% of what we perceive as taste is due to smell. And the mere smell of certain foods can stimulate hunger and the production of digestive juices. Thus, simple nasal maintenance, such as daily nasal cleansing, is an important part of good intestinal health — not to mention the fact that it washes out vast quantities of bacteria and viruses, thus preventing them from entering the digestive tract. Incidentally, the primary role of the uvula, the fleshy piece that hangs from the back of the throat, is to detect food that passes over it, and rise up during swallowing to close off the nose from the food so it can’t back up into the nose.
Salivary glands
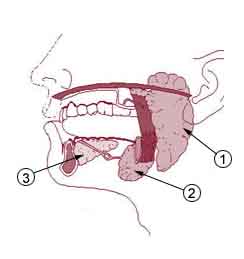 There are three pairs of salivary glands that secrete saliva, the first of the digestive juices to contact the food in the mouth. They are:
There are three pairs of salivary glands that secrete saliva, the first of the digestive juices to contact the food in the mouth. They are:
- The parotid glands, which are located high up in each cheek, just below the ears. Incidentally, these are the glands that gets infected and swell up when you have the mumps.
- The submandibular glands, which are located in the floor of the mouth just below the parotid glands.
- And the sublingual glands, which are located on the floor of the mouth, upfront.
Saliva performs several key functions. It moistens the mucous membrane, moistens food for easy swallowing, lubricates the esophagus for swallowing, washes the mouth, kills bacteria, dilutes poisonous substances, and contains enzymes that begin the digestion process. Your body produces from 1-1.5 liters of saliva per day (about a quart). More than 99% of that saliva is water, and almost all of it is reabsorbed in the digestive tract. The tiny bit of saliva that is not water contains about 0.05% enzymes:
- Lysozyme kills bacteria in the mouth. Incidentally, your mouth is remarkably dirty and infested with bacteria — some good, but most not so much. It is really true that the mouth of a dog that drinks from the toilet is cleaner than yours. And if you must be bitten, better to be bitten by a dog than a person.
- Lingual lipase breaks triglycerides down into far healthier and more easily digested fatty acids and monoglycerides.
- And then there’s salivary amylase
Salivary amylase begins the breakdown of carbohydrates
Your digestive system is remarkably adaptable; after all, it can handle pepperoni pizza, beer, and Ding Dongs. But there are consequences if you abuse it. There are two forms of abuse. First, there’s eating a diet high in cooked and processed food that has destroyed all of the enzymes naturally present in the food. In this particular case, we’re talking about amylase. All natural carbohydrates contain the amylase needed to digest them. In fact, the amylase found in wheat and other grains will actually work in the stomach at high acid pH levels of 3 to 4. If natural amylase is present, it will handle a great deal of the digestive process required to break down the carbohydrates you eat. Second, you need to chew your food thoroughly. If you chew your food well enough, it slows down the entire eating process, which spreads out the glycemic response. It also allows the amylase in the saliva to effectively start breaking down the carbohydrates, which takes a huge burden off your pancreas. And it allows time for your stomach to signal your brain that you’re full (it normally takes twenty minutes for your brain to catch up with your stomach), so you end up eating less.
So, how much do you need to chew your food? There’s an old saying: “You should drink your solids and chew your liquids.” What that means is that you should chew the dry food you eat until it turns to liquid in your mouth (about forty chews per mouthful), and that you should swish liquids back and forth in your mouth (chew them as it were) an equal number of times. This helps mix enzymes into the food or liquid and begins the digestive process.
The more you chew, the more effective these enzymes are.
And if you don’t do these things, how much does the body have to compensate? Amylase levels in the saliva of people eating the typical western cooked/processed diet are as much as 40 times higher than that found in people eating a more natural diet!
Note: During dehydration, the brain signals the mouth to stop the flow of saliva to impel us to drink more water and to conserve fluids.
Swallowing (deglutition)
Once you start chewing your food and mixing it with saliva, it picks up a technical name; the wad of chewed food is called a bolus. During the voluntary stage of swallowing, the tongue moves the bolus of food upward and backward. Once the bolus reaches the back of the throat, all actions become involuntary — they happen outside of your conscious control. During the first of these involuntary phases, the muscles move the food down and back into the esophagus. And finally, the food is actively moved through the esophagus to the stomach. By actively, I’m referring to the fact that movement through the esophagus is the result of series of active, coordinated movements by constrictor muscles lining the esophagus — not the result of gravity. Specifically, longitudinal muscles pull the esophagus up and relax lower portions so that the circular bands of muscle lining the esophagus can constrict and move the bolus down into the stomach. In fact, although it is not advisable, you can easily swallow when hanging upside down.
As we discussed in our series on breathing, aspiration (entry of food or water) into the lungs and nasopharynx is prevented in a series of involuntary actions.
- The uvula and soft palate move upward to close off the nasopharynx.
- The larynx is pulled forward and upward under the protection of the tongue.
- The epiglottis moves back and down to close the opening of the trachea and airway.
- Food slides over the epiglottis into the esophagus.
- Vocal cords close to further block the airway.
- Breathing ceases for about 2 seconds while this process takes place, then resumes.
Esophagus (“carries food”)
Although there are a number of things that can go wrong with the esophagus, they are mostly medical and fall outside the scope of our discussion. For our purposes, the only function of the esophagus is to carry food from the mouth to the stomach. No digestion or absorption of nutrients takes place in the esophagus. Liquids pass through quickly — in about a second. A food bolus, on the other hand will take about five to nine seconds to make its way through the esophagus.
In fact, there is little to interest us from an alternative health point of view until we reach the lower esophageal sphincter, which is located at the end of the esophagus just above the diaphragm. The sphincter is not actually an anatomical structure. It’s just an area at the end of the esophagus that is capable of constricting to effectively separate the stomach from the esophagus. When functioning properly, it allows food to enter the stomach while at the same time preventing stomach acids and bile from refluxing back into the esophagus.
From a medical point of view, there are a number of things that can go wrong with the lower esophageal sphincter, such as achalasia (inability to relax), which prevents food from entering the stomach. But for the purposes of our discussion, two conditions stand out: GERD and hiatal hernia. These conditions used to be handled surgically, but with rather poor results. Antacids provided temporary relief, but as we will learn when we discuss the stomach, actually aggravated the problems. Now, new drugs called proton pump inhibitors are the treatment of choice. They work by cutting the ability of the body to produce stomach acid and are more effective, from a medical point of view, than either surgery or antacids.
GERD
GERD (Gastro esophageal reflux disease) is also known as acid reflux disease. It is a condition in which the sphincter fails to prevent acid from backing up into the esophagus. This causes inflammation, scarring, and can lead to esophageal cancer. We will talk more about GERD when we talk about acid production in the stomach, which is the primary contributing factor in this disease. We will also discuss why Prilosec, Prevacid, and Nexium may not be the best answers to this problem. One other note on acid reflux at this time is that hiatal hernia is often a contributing factor.
Hiatal hernia
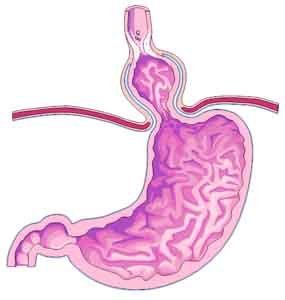 Hiatal hernia is a condition in which part of the stomach moves above the diaphragm, into the chest. They are much more common than generally recognized and can produce a wide variety of symptoms that make diagnosis difficult. Hiatal hernias can manifest as severe chest pains that mimic a heart attack, pressure in the chest, or severe stomach pain. And most notably, as mentioned above, a hital hernia can significantly aggravate acid reflux as it pushes the esophageal sphincter out of position, thereby seriously compromising its ability to prevent stomach acid from moving into the esophagus.
Hiatal hernia is a condition in which part of the stomach moves above the diaphragm, into the chest. They are much more common than generally recognized and can produce a wide variety of symptoms that make diagnosis difficult. Hiatal hernias can manifest as severe chest pains that mimic a heart attack, pressure in the chest, or severe stomach pain. And most notably, as mentioned above, a hital hernia can significantly aggravate acid reflux as it pushes the esophageal sphincter out of position, thereby seriously compromising its ability to prevent stomach acid from moving into the esophagus.
There are very few medical options for treating a hiatal hernia. As I mentioned earlier, surgical intervention is only marginally effective. The common medical approach today is to reduce the amount of acid the stomach produces with proton pump inhibitor drugs. But the use of these drugs is even more questionable for a hiatal hernia than for standard GERD as it does nothing at all to alleviate the underlying condition — the fact that part of your stomach is now up in your chest cavity. It merely helps control one symptom.
Fortunately, there are alternatives.
- Self massage
- Chiropractic adjustment
- Then, once you’ve corrected the initial hiatal hernia you might want to do some yoga exercises to strengthen your diaphragm so that your stomach won’t slip back up through the opening again. For example:
Conclusion
That concludes our introduction to the digestive system — getting food into the stomach. In our next issue, we will cover the stomach in detail. Areas of interest will include:
- The need for enzymatic digestion
- Why proton pump inhibitor drugs create at least as many problems as they resolve
- How stomach acid is produced in your body and how to use that feedback loop to your advantage
- Why antacids create more acid than they get rid of
- Peptic ulcers and how to get eliminate them
- The proper way to eat to control appetite
- The types of food your stomach is anatomically designed to handle
- The feedback loop that drains your body of enzymes
- And much more
Continue reading Jon’s series about digestive health:
Your Stomach, Part 1
Your Stomach, Part 2
Your Stomach, Part 3








Thanks for another great post
Thanks for another great post John. I was looking for something specific, and it just happened to be the very condition you said would not be discussed in this post: achalasia. Any chance of addressing it in a featured blog as part of this continued series on digestive health? From what I’ve read there is no known (allopathic/medical!!!) cure for it and treatment is merely to reduce dysphagia and to decrease esophageal pressure.
There are no (again, medical) interventions available that can restore esophageal peristalsis, and I am aware of someone who smokes 2/3 cigarettes before eating as the ONLY remedy for relaxing the oesophageal sphincter. That way he can eat without too much discomfort. Otherwise it’s too restrictive and painful to eat. So generally he doesn’t eat!
As you know, treatment includes pharmacological, endoscopic, and surgical modalities. But the procedures usually make patients nothing more than veritable lab rats, with patients often complaining of being in constant pain (on a 10-point scale being an eight 24/7/365 is common).
My question is: what causes achalasia, and is there a completely naturopathic treatment protocol you could suggest that would leave the immune system intact and actually restore esophageal peristalsis to normalcy? I’m aware of the limited benefits of light therapy, but do you have other more beneficial suggestions?
Warmest regards in your endeavours to spread the Wellness Gospel,
Chevannes
Warmest regards to you,
Chevannes
It’s usually caused by nerve
It’s usually caused by nerve damage – often as the result of a minor injury to the neck or upper spine. Unfortunately, there is no foolproof treatment. You might want to consider chiropractic treatment in case the nerves are only impinged, and not actually damaged. It would also be worthwhile searching to see if anyone is developing a biofeedback treatment – since biofeedback holds out the possibility of learning to exercise conscious control over involuntary muscles. Then again, if the root cause is nerve damage, then that is unlikely to help.
There is no dicussion about
There is no dicussion about the benefits of ingesting a super food blended smoothie. How does this mixture speed thru the digestive process and how is beneficial, such as, for lessening the need for digestive enzymes
A “super food blended
A “super food blended smoothie,” unless you’re putting something very unusual in it, is still a blend of proteins, fats, and carbohydrates. How those are digested is covered in complete detail in the rest of the series on the digestive system. The newsletter above is merely an overview/introduction to how digestion works. As you can see in the links at the bottom of the newsletter, there are three additional newsletters on the stomach alone – plus even more on the small intestine, large intestine, not to mention the organs of digestion. As to enzymes, it all depends on what you’re making your smoothie from. The more alive the ingredients are, the less the need for digestive enzymes. The more processed or exposed to heat they’ve been, the more digestive enzymes you need. How digestive enzymes work is covered throughout the series on the digestive tract – as is required because different enzymes do different things in different parts of the digestive tract.
Thank you. Please let me be
Thank you. Please let me be more specific. I am preparing smoothies with aspargus, spinach, smetimes kale, peas, walnuts, brazil nuts, pumpkin seeds, extra virgin coconut oil, saurkraut, celery, and then add some spices ( tumeric, ginger, cilantro, garlic, cayenne, cinnamin) – all USDA organic ingredients. I sometimes add pineapple, and always include a super food formula in the mix, but this formula is added rather than blended. I also add the sprouted barley. With this in mind, how would any digestive enzymes help or be necessary to assist with digestion? Specifically, is the speed of digestion improved by this type of meal? I am very persuaded by your presentation that enzyme function needs to be supported. Maybe when I eat fish? Maybe when I eat cheese? I am trying to identify the types of foods that need the extra help, either alone or because they are combined with nuts, fruits, etc.? Also, I am starting the proteolytic enzymes between meals to ehance my health. I am asking about the digestive enzymes primarily in reference to increasing the speed of digestion – quicker would be better since it would involve less enzyme time and effort. Thank you again for the instructive article.
As described, your smoothie
As described, your smoothie contains mostly live foods so it will have a lot of enzymes present to aid in its own digestion. However, you did not talk about “how” you drink it. As Jon Barron says, “You need to drink your solids and chew your liquids.” You need to chew your solid food enough so that it liquefies in the mouth – and you need to chew your liquids as though they were solids. In other words, you need to swish the smoothie around in your mouth to thoroughly mix it with saliva, which contains the amylase necessary for digestion of the carbohydrates. Otherwise, it will be amylase deficient when it enters your stomach. In general, chewing solid food 40 times per mouthful and swishing liquid foods 40 times per mouthful is the ideal.
All of that said, taking a digestive enzyme with your smoothie can only add digestive enzymes to the mix, improve digestion, and take stress off your pancreas. In other words, although less necessary than with many meals, it will still be highly beneficial.
Note: sometime, for fun, you might want to try the oatmeal test described near the end of Jon’s newsletter on The Enzyme Story. Once you run the test, what digestive enzymes do will no longer be theoretical for you.
I can guarantee you that in
I can guarantee you that in the future, I will be “thoroughly” chewing my smoothies!
Can digestive enzymes cause
Can digestive enzymes cause the pancreas and gallbladder to become lazy? I was taking them for years. When i adopted a raw vegan diet, i stopped taking them. I recently (approx 7m after adopting a raw vegan diet, from a GAPS-like diet (horrible diet, btw)), it was DX'd that my pancreas/gallbladder are insufficiently producing enzymes/insulin. When i was eating meat, i had to take 3 different types of enzymes plus HCl…and even those werent enough to help me digest cooked foods and meat. I digest better as a raw vegan, but its still not optimal (i have UC and dysbiosis). So, could digestive enzymes have caused my lazy pancreas and GB? Would enzymes help? Or is there another way instead, like somehow strengthen and support those organs in restoring their function? Lastly, what does Jon feel is a human's natural diet? Fruitarian (fruit, greens, nuts seeds)? Vegan (same as the former but with grains, legumes)? Ovo-veg? Lacto? Pesco? Meat? Paleo/primal? And what is the proper macronutrient ratio (low fat like 80-10-10 or zone or high fat….)? Thanks!
If you rephrase the question,
If you rephrase the question, it answers itself.
Is every animal (other than man) making their pancreas and gallbladder lazy because they naturally eat raw foods filled with live enzymes? Let’s hear it for McDonalds then because a diet of 100% cooked and processed foods, totally devoid of enzymes, would obviously strengthen your digestive system. Yes?
Bottom line: we use supplemental digestive enzymes to compensate for the enzyme dead foods we eat. Considering that most Americans don’t use supplemental enzymes and still have digestive problems as they age, I think you need to look elsewhere for the cause of the problem.
There is a false process of
There is a false process of elimination logic here. The fact that Incisors are used for grasping prey and that we don’t have them isn’t telling of a non-carniverous diet. It is an indication that the energetic needs and calcium needs of large incisors went away after we went to a tool based system of hunting.