
We’ve previously explored the importance of testosterone in depth. It provides energy and zest for life, increases muscle mass and decreases fat, and improves libido and sex performance. As your testosterone levels drop over time, all of those benefits do a 180 and go into the negative. In other words, you start aging at an accelerated rate. Today, however, we’re going to look at some different aspects that weren’t covered in that newsletter. We’re also going to examine the issue of free VS bound testosterone in more detail. And we’re then going to look at some recent studies and what they have to say about the benefits and risks of actual testosterone supplementation–as well as the truth behind them. And finally, we’re going to take a look at how, in most cases, you can maximize the benefits and minimize the risks associated with testosterone supplementation by instead reactivating your body’s ability to produce its own testosterone and optimizing your levels of bioavailable testosterone VS adding testosterone with a doctor’s prescription.
What Is Testosterone?
Testosterone, which is synthesized from cholesterol in your bloodstream, is the major circulating androgen hormone in men. The approximately 500 million Leydig cells in the testes secrete more than 95% of the 6-7 mg of testosterone produced per day in the male body. (To understand how much that actually is, you can think of it as the amount of supplement you would find in a mere 1/10th of an average capsule–literally, just a pinch.) The rest is produced by the adrenal glands. In women, the ovaries account for half of the testosterone in the body; and as with men, the adrenal glands account for most of the rest. Women have a much smaller amount of testosterone in their bodies compared to men, but, regardless, testosterone plays an equally crucial role throughout the body in both men and women. It affects the brain, bone and muscle mass, fat distribution, vascular system, energy levels, genital tissues, and sexual functioning.
So how much testosterone should you have?
As do most numbers in the human body, normal values for testosterone fall within a reference range and are just a guide. Numbers that fall outside the range do not necessarily mean there’s a problem–just an indication that there might be. One reason for this looseness is that ranges vary from lab to lab, and each lab sets its own range for what’s normal. There’s also a second, more important reason, but we’ll talk about that later. The bottom line is that your doctor will evaluate your test results based on your overall health as well as other factors. This means that a value that falls outside the normal values listed below may still be normal for you–or your lab.
| Total testosterone: Average normal results across multiple laboratories | |
| Men | 270-1070 ng/dL (9-38 nmol/L) |
| Women | 15-70 ng/dL (0.52-2.4 nmol/L) |
At this point, a question might have occurred to you. If the male body is producing 6-7 mg of testosterone a day, but there’ only 270-1070 ng/dl in the bloodstream, where’s the rest of it going? And the answer is that testosterone, which is metabolized from cholesterol, is itself metabolized into various 17-ketosteroids, of which there are a bunch. For example, testosterone can be metabolized to dihydrotestosterone (“DHT”) by the enzyme 5-alpha-reductase or to estradiol (“E2”) by an aromatase enzyme complex. In any case, the small amount that shows up in your bloodstream when tested is what’s left. This also means that simply adding testosterone to your body to increase your numbers may not produce quite the results you and your doctor are looking for if your body converts most of that added testosterone to estrogen and DHT.
It’s also important to keep in mind that testosterone declines with age. In fact, the age-related decline of testosterone has been confirmed in several cross-sectional and longitudinal studies and results from dysfunction in the hypothalamic-pituitary-testicular axis.1 Feldman HA, Longcope C, Derby CA, et al. “Age trends in the level of serum testosterone and other hormones in middle-aged men: longitudinal results from the Massachusetts Male Aging Study.” J Clin Endocrinol Metab. 2002 Feb;87(2):589-98. http://www.ncbi.nlm.nih.gov/pubmed/11836290 , 2 Wu FC, Tajar A, Pye SR, et al. “Hypothalamic-pituitary-testicular axis disruptions in older men are differentially linked to age and modifiable risk factors: the European Male Aging Study.” J Clin Endocrinol Metab. 2008 Jul;93(7):2737-45. http://www.ncbi.nlm.nih.gov/pubmed/18270261 , 3 Harman SM, Metter EJ, Tobin JD, et al; “Baltimore Longitudinal Study of Aging. Longitudinal effects of aging on serum total and free testosterone levels in healthy men. Baltimore Longitudinal Study of Aging.” J Clin Endocrinol Metab. 2001 Feb;86(2):724-31. http://www.ncbi.nlm.nih.gov/pubmed/11158037 Studies have shown that total testosterone decreases by approximately 30% in healthy men between the ages of 25 and 75. And free testosterone levels decline even more significantly with decreases of approximately 50% being typical.4 Moffat SD, Zonderman AB, Metter EJ, et al. “Longitudinal assessment of serum free testosterone concentration predicts memory performance and cognitive status in elderly men.” J Clin Endocrinol Metab. Nov 2002; 87 (11): 5001-5007. http://www.ncbi.nlm.nih.gov/pubmed/12414864 , 5 Morley JE, Kaiser FE, Perry HM, et al. “Longitudinal changes in testosterone, luteinizing hormone, and follicle-stimulating hormone in healthy older men.” Metabolism. Apr 1997 ;46 (4): 410-413. http://www.ncbi.nlm.nih.gov/pubmed/9109845 , 6 Araujo AB, O’Donnell AB, Brambilla DJ, et al. “Prevalence and incidence of androgen deficiency in middle-aged and older men: estimates from the Massachusetts Male Aging Study.” J Clin Endocrinol Metab. Dec 2004; 89 (12): 5920-5926. http://www.ncbi.nlm.nih.gov/pubmed/15579737 But most importantly, bioavailable testosterone declines even more.
Another factor to consider is that testosterone levels for postmenopausal women are about half the normal level for a healthy, nonpregnant woman. And a pregnant woman will have 3 to 4 times the amount of testosterone compared to a healthy, nonpregnant woman.
Additionally, it should be noted that testosterone levels vary from day to day–and even from hour to hour. They are constantly being regulated and fine-tuned by your body and are usually highest in the morning and lowest in the evening.
And finally, take note of the size of the range (see table above) in terms of defining “normal” levels of testosterone. For both men and women, it’s essentially a fourfold spread between the low and high normal numbers. That’s huge! Which brings up the questions:
- Why is the spread so large?
- How can such wildly varying numbers produce similar “normal” physiological results in different bodies?
There are two parts to the answer, and we’ll cover both parts a little later.
The Key Thing to Understand About Testosterone
 And now we come to the most important section in this newsletter. We’re going to look at what those numbers actually tell us, and it’s probably not what you think. So, what do they mean? To answer that, we first need to answer the question: what the heck is an ng/dl–after all, a thousand of them sure sounds like a lot? But as it turns out, ng/dl stands for nanograms per deciliter. A nanogram is a billionth of a gram, and a deciliter is a 10th of a liter, which still probably doesn’t mean a lot to you. So, let’s give it some context. There are approximately 5 liters of blood in the human body. That’s 50 deciliters. In other words, there are anywhere from approximately 14,000-50,000 nanograms worth of testosterone in the average blood supply of a bulked-up, hairy-chested, fully-muscled, deep-voiced man, and that certainly sounds like a lot. (For the average women, we’re talking about a fraction of that, of course–750-3,500 nanograms.) But again, a nanogram is a billionth of gram. If you translate that 50,000 nanograms to milligrams (that’s thousandths of gram), you get just 0.05 milligrams. That’s not even 1 milligram. That’s just 5/100ths of a milligram. To understand how small an amount this really is, let’s again consider your average supplement capsule.
And now we come to the most important section in this newsletter. We’re going to look at what those numbers actually tell us, and it’s probably not what you think. So, what do they mean? To answer that, we first need to answer the question: what the heck is an ng/dl–after all, a thousand of them sure sounds like a lot? But as it turns out, ng/dl stands for nanograms per deciliter. A nanogram is a billionth of a gram, and a deciliter is a 10th of a liter, which still probably doesn’t mean a lot to you. So, let’s give it some context. There are approximately 5 liters of blood in the human body. That’s 50 deciliters. In other words, there are anywhere from approximately 14,000-50,000 nanograms worth of testosterone in the average blood supply of a bulked-up, hairy-chested, fully-muscled, deep-voiced man, and that certainly sounds like a lot. (For the average women, we’re talking about a fraction of that, of course–750-3,500 nanograms.) But again, a nanogram is a billionth of gram. If you translate that 50,000 nanograms to milligrams (that’s thousandths of gram), you get just 0.05 milligrams. That’s not even 1 milligram. That’s just 5/100ths of a milligram. To understand how small an amount this really is, let’s again consider your average supplement capsule.
- That little capsule is 500 milligrams (half a gram).
- So, to get it down to 1 milligram (1/1000 of a gram), we have to take just one 500th of that, which would be just a few grains of whatever is in the capsule.
- But that’s still way more than what we’re talking about. Remember, at the high end, we’re talking about just 0.05 milligrams, not 1 milligram.
- To actually get to the amount we’re talking about, you have to take just 5/100 of those few grains–which would be less than you can see with the naked eye. And that miniscule amount is how much testosterone is circulating in the most Neanderthal-DNA-expressing man you can find. It’s their Total T level. And for most men, it’s half of that or less. And for most women, it’s 1/10 of it.
The bottom line, and the key point you need to understand, is that it requires just a fraction of even that minuscule amount to dramatically change the impact of testosterone on your body. We’re NOT talking about ounces or grams or even drops. We’re talking about infinitesimal changes having dramatic impact on your health outcome.
So, with that understanding in mind, let’s continue.
How Testosterone is Regulated in the Human Body
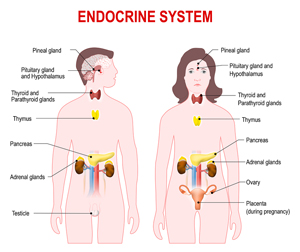 The pituitary gland produces two hormones that trigger production of testosterone in the Leydig cells of the testes in men and in the ovaries of women. Luteinizing hormone (“LH”) plays the primary role, and follicle stimulating hormone (“FSH”) the secondary role. But as with most hormonal messaging systems in the body, LH and FSH are part of a feedback loop. The feedback loop involves testosterone inhibition of FSH and LH. In other words, low testosterone levels in the bloodstream trigger the pituitary to release LH and FSH, which causes the testes and ovaries to produce more testosterone. Then, as testosterone levels in the bloodstream rise, that signals the pituitary to stop releasing LH and FSH, which stops production of testosterone.
The pituitary gland produces two hormones that trigger production of testosterone in the Leydig cells of the testes in men and in the ovaries of women. Luteinizing hormone (“LH”) plays the primary role, and follicle stimulating hormone (“FSH”) the secondary role. But as with most hormonal messaging systems in the body, LH and FSH are part of a feedback loop. The feedback loop involves testosterone inhibition of FSH and LH. In other words, low testosterone levels in the bloodstream trigger the pituitary to release LH and FSH, which causes the testes and ovaries to produce more testosterone. Then, as testosterone levels in the bloodstream rise, that signals the pituitary to stop releasing LH and FSH, which stops production of testosterone.
All well and good, but how much testosterone you have circulating in your bloodstream is only part of the equation. The other part is how much of that can your body actually use.
As much as 98% of the testosterone circulating in the blood is bound to protein. In men, approximately 40% of the binding is to the high-affinity sex hormone binding globulin (“SHBG”). The remaining 60% is bound weakly to albumin. But what does that mean?
The term “free” testosterone (Free T) refers to the fraction of testosterone in the blood that is not bound to protein. The term “total testosterone” (Total T) refers to the free testosterone plus the protein-bound testosterone circulating in the blood–in other words, all of it. But neither of those numbers get us where we really need to be. Perhaps the most important number to keep in mind–and the one least tested for by doctors–is “bioavailable testosterone.” Bioavailable testosterone refers to the non-SHBG bound testosterone–in other words, the combination of free testosterone plus the testosterone weakly bound to albumin. This is important because the testosterone bound to albumin can easily be converted by the body back to free testosterone as needed whereas the testosterone bound to SHBG, not so much. Another way to think about this is that free testosterone is like cash in your pocket. Albumin bound testosterone is like money in the bank that you can easily draw on from an ATM whenever you need more. And SHBG bound testosterone is like money in a hard asset like a house, which can only be accessed with great difficulty. It’s there, but tough to get to.
Note: SHBG concentrations are normally high in children of both sexes. After puberty, SHBG levels decrease more rapidly in males than in females. Levels are normally stable in adults and then begin to increase in the elderly male at the same time that total testosterone levels begin to decrease. In postmenopausal women, SHBG, testosterone, and estrogen concentrations decrease as hormone production by the ovaries tapers off.
Measuring Testosterone
Usually, Total T is the first test ordered when symptoms indicate low testosterone levels, but numbers from this test can be misleading since it doesn’t account for how much testosterone is actually available for use by the body. (It should also be noted that false Total T readings are more likely in older or obese patients.) Free T, therefore, is the more useful number when there is a reason to suspect that there may be a problem. In any case, Free T numbers, although better than Total T numbers, can still wildly miss the mark since they don’t differentiate between albumin bound testosterone, which is easily available for use by your body, and SHBG bound testosterone, which is not. So once again, the number we truly want is the level of bioavailable testosterone–the combination of free testosterone and albumin bound testosterone. So, how do we get there?
How are testosterone levels actually determined–especially considering how little there is to detect? And, in fact, only total testosterone is routinely measured. Free and bioavailable testosterone are not usually measured but, rather, calculated from the total testosterone results and from formulaic estimates as to how much SHBG and albumin are in the blood. While it is true that Free T can be measured directly using equilibrium dialysis, ultrafiltration or steady state gel filtration, all these methods are lengthy, require a high degree of skill and are unsuited to routine use. Direct measurement of Free T is pretty much only used in clinical studies. Instead, Free T is calculated using set formulas.
So, how do we actually measure Total T. The quick and dirty method for establishing Total T levels is immunoassays, and although they are widely used, they are not reliable, especially at low concentrations. Liquid chromatography tandem mass spectrometry (LC-MS/MS) has become the method of choice for steroid hormone measurements.7 Rosner W, Auchus RJ, Azziz R, et al. “Position statement: Utility, limitations, and pitfalls in measuring testosterone: an Endocrine Society Position Statement.” J Clin Endocrinol Metab. 2007;92:405-413. http://www.ncbi.nlm.nih.gov/pubmed/17090633 But even here, things are not necessarily straightforward. Yes, LC-MS/MS requires only small sample volumes and offers fast analysis times, but it is much more complex, and its accuracy is dependent in the skill of the lab tech in preparing the samples for testing and thus can vary notably from test to test.
As I mentioned a moment ago, free testosterone and bioavailable testosterone are not normally measured in patients, but rather calculated–and this is where accuracy gets even dicier. Using this method, the lab simply applies a formula based on population averages to estimate the levels of albumin and SHBG in the blood, based on age and sex, and then calculates free and bioavailable testosterone as follows:
- Free testosterone = Total T — (SHBG bound T) — (albumin bound T)
- Bioavailable testosterone = Total T — (SHBG bound T)
For these calculations to work, though, since they are not based on measurement but by applying a formula, it requires that the formula’s estimates concerning SHBG and albumin, and how much of the testosterone they are actually binding, be constant across all individuals. In other words, it assumes the formula works for everyone. The problem is that although the formulaic estimates tend to be somewhat consistent across populations, they are not necessarily consistent when it comes to individuals. Or to put it another way: “peoples is different.” In any case, the bottom line is that although total testosterone can be measured somewhat accurately, the more important numbers for free and bioavailable testosterone are merely estimated with somewhat variable accuracy.
Incidentally, our discussion of Total T, Free T, and Bioavailable T provides the first half of our answer as to why the normal range for testosterone in the bloodstream is so large. As we’ve just learned, Total T provides very little useful information as to what’s really happening in your body. Depending on the unique ratios connecting Total T, Free T, and Bioavailable T, a man with just 300 ng/dl of testosterone could actually have just as much Bioavailable T as a man with 1000 ng/dl–and thus, identical physiological outcomes. And as we’ve discussed, different bodies are anything but standard, and it doesn’t take a huge difference in the percentage of SHBG that is actually binding testosterone from one body to the next to drastically change the ratios. But beyond that, there are two huge jokers in the deck that provide the second half of our answer, and we’ll cover them in a bit. But before we go there, let’s take a look at the two new testosterone studies that triggered this newsletter in the first place.
Two Testosterone Studies
 The first study that we’re going to look at was published in the Journal of the American Medical Association in February of this year.8 Resnick SM, Matsumoto AM, Stephens-Shields AJ, et al. “Testosterone Treatment and Cognitive Function in Older Men With Low Testosterone and Age-Associated Memory Impairment.” JAMA. 2017;317(7):717-727. http://jamanetwork.com/journals/jama/article-abstract/2603930 It was designed to explore the question of whether or not treatment with testosterone was associated with improved memory in older men with low testosterone and age-associated memory impairment? Most cognitive functions decline with age, and some studies have “suggested” that testosterone treatment might improve these functions.9 Ciocca G, Limoncin E, Carosa E, Di Sante S, et al. “Is Testosterone a Food for the Brain?” Sex Med Rev. 2016 Jan;4(1):15-25. doi: 10.1016/j.sxmr.2015.10.007. http://www.ncbi.nlm.nih.gov/pubmed/27872000 , 10 Jung HJ, Shin HS. “Effect of Testosterone Replacement Therapy on Cognitive Performance and Depression in Men with Testosterone Deficiency Syndrome.” World J Mens Health. 2016 Dec;34(3):194-199. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC5209560/ Unfortunately, the new study concluded that testosterone therapy provided NO benefit over placebo when it came to subjective memory complaints and actually impaired performance on tests of verbal and visual memory. The headlines pretty much tell you how the health media ran with the story.
The first study that we’re going to look at was published in the Journal of the American Medical Association in February of this year.8 Resnick SM, Matsumoto AM, Stephens-Shields AJ, et al. “Testosterone Treatment and Cognitive Function in Older Men With Low Testosterone and Age-Associated Memory Impairment.” JAMA. 2017;317(7):717-727. http://jamanetwork.com/journals/jama/article-abstract/2603930 It was designed to explore the question of whether or not treatment with testosterone was associated with improved memory in older men with low testosterone and age-associated memory impairment? Most cognitive functions decline with age, and some studies have “suggested” that testosterone treatment might improve these functions.9 Ciocca G, Limoncin E, Carosa E, Di Sante S, et al. “Is Testosterone a Food for the Brain?” Sex Med Rev. 2016 Jan;4(1):15-25. doi: 10.1016/j.sxmr.2015.10.007. http://www.ncbi.nlm.nih.gov/pubmed/27872000 , 10 Jung HJ, Shin HS. “Effect of Testosterone Replacement Therapy on Cognitive Performance and Depression in Men with Testosterone Deficiency Syndrome.” World J Mens Health. 2016 Dec;34(3):194-199. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC5209560/ Unfortunately, the new study concluded that testosterone therapy provided NO benefit over placebo when it came to subjective memory complaints and actually impaired performance on tests of verbal and visual memory. The headlines pretty much tell you how the health media ran with the story.
“No difference in cognitive impairment seen in men on testosterone treatment.” Healio.11 No difference in cognitive impairment seen in men on testosterone treatment.” Healio February 24,2017. (Accessed 5 Mar 2017.) http://www.healio.com/internal-medicine/mens-health/news/online/%7B9b21ef00-301b-4647-bf5f-fd66b03e973a%7D/no-difference-in-cognitive-impairment-seen-in-men-on-testosterone-treatment
“Case Closed: Testosterone Does Not Boost Cognition.”, ALZFORUM.12 “Case Closed: Testosterone Does Not Boost Cognition.” ALZFORUM. 24 Feb 2017. (Accessed 5 Mar 2017.) http://www.alzforum.org/news/research-news/case-closed-testosterone-does-not-boost-cognition
Case closed? Not necessarily. There was another study published less than a year ago in CNS & Neurological Disorders Drug Targets that came to a notably different conclusion. This one, curiously, was largely ignored by the media.
This study determined that, when comparing baseline Mini Mental State Examination (MMSE) scores, participants receiving testosterone supplementation showed a modest but “significant” improvement with testosterone supplementation.13 Wahjoepramono EJ, Asih PR, Aniwiyanti V, Taddei K, Dhaliwal SS, Fuller SJ, Foster J, et al. “The Effects of Testosterone Supplementation on Cognitive Functioning in Older Men.” CNS Neurol Disord Drug Targets. 2016;15(3):337-43. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC5078598/ In contrast, no significant changes in MMSE scores were observed following placebo treatment. Additionally, depression scores significantly decreased following testosterone treatment, and the observed improvement maintained over time, even after treatment was stopped. Different studies; different results; different conclusions; only one was covered by the media.
And speaking of the media, their stories and headlines ignored the fact that improved cognitive function is not one of the primary benefits normally associated with testosterone therapy. Rather, if it had turned out to be true–or eventually turns out to be true as suggested by the CNS study–it would be a nice bonus benefit. (Fortunately, there are a number of non-testosterone, natural alternatives for improving cognitive function that have already been proven to work in studies.)
Which brings us to the second study, also published in JAMA in February of this year.14 Budoff MJ, Ellenberg SS, Lewis CE, et al. “Testosterone Treatment and Coronary Artery Plaque Volume in Older Men With Low Testosterone.” JAMA. 2017;317(7):708-716. http://jamanetwork.com/journals/jama/article-abstract/2603929 This study attempted to determine if testosterone treatment of older men with low testosterone would produce a decrease in noncalcified coronary artery plaque volume? Instead, the study found that testosterone therapy was associated with a significant increase in noncalcified coronary artery plaque volume. Not surprisingly, the health media ran with that factoid, leading with headlines such as:
Atherosclerosis Speeds Up in Older Men on Testosterone: T Trial. Medscape.15 Marlene Busko. “Atherosclerosis Speeds Up in Older Men on Testosterone: T Trial.” Medscape February 24, 2017. (Accessed 5 Mar 2017.) http://www.medscape.com/viewarticle/876214
Before we move on, it’s probably worth quoting the last sentence in the study’s results section–almost a throwaway line that was not mentioned in any of the media coverage. “No major adverse cardiovascular events occurred in either group.” In other words, the increased plaque did not cause any observable health problems–at least during the one year run of the study. What could explain that?
 Well, as with the cognitive/testosterone study, there’s more to the story. First, there have been several recent studies that offer a counter narrative. For example, there was the study published just a couple of months earlier in the Indian Heart Journal16 Kunal Gururani, , John Jose, and Paul V. George. “Testosterone as a marker of coronary artery disease severity in middle aged males.” Indian Heart Journal, 2016-12-01, Volume 68, Pages S16-S20. http://www.clinicalkey.com/#!/content/playContent/1-s2.0-S0019483216302607 that found that patients with coronary artery disease had significantly lower levels of total serum testosterone, free testosterone, and bioavailable testosterone when compared to controls. And perhaps more to the point, the study also showed that levels of total, free, and bioavailable testosterone correlated positively with both the dilation of, and blood flow through, the brachial artery.
Well, as with the cognitive/testosterone study, there’s more to the story. First, there have been several recent studies that offer a counter narrative. For example, there was the study published just a couple of months earlier in the Indian Heart Journal16 Kunal Gururani, , John Jose, and Paul V. George. “Testosterone as a marker of coronary artery disease severity in middle aged males.” Indian Heart Journal, 2016-12-01, Volume 68, Pages S16-S20. http://www.clinicalkey.com/#!/content/playContent/1-s2.0-S0019483216302607 that found that patients with coronary artery disease had significantly lower levels of total serum testosterone, free testosterone, and bioavailable testosterone when compared to controls. And perhaps more to the point, the study also showed that levels of total, free, and bioavailable testosterone correlated positively with both the dilation of, and blood flow through, the brachial artery.
But second and more important, it needs to be remembered that testosterone therapy as practiced, in this case with a gel patch, is essentially a blunt-force protocol. Remember, as we discussed earlier, it takes very little additional testosterone in the bloodstream to make a huge difference in health outcomes, and if your body is functioning properly, this is being regulated on a minute by minute basis by the feedback loop between the pituitary gland and the glands that produce testosterone (the testes and the ovaries). Using a gel patch makes for much wilder swings in levels and much less subtlety in terms of minute-by-minute self-regulation. And finally, while testosterone therapy may make a large difference in your body’s total testosterone numbers, it’s not particularly nuanced in terms of how that testosterone apportions itself vis-à-vis total, free, and bioavailable levels.
Further, the relationship between testosterone levels and heart disease is actually quite complex. As explained in an issue of Harvard Health Publications:
“In high doses, androgens tend to raise LDL (“bad”) cholesterol levels and lower HDL cholesterol levels. That’s one of the things that gave testosterone its bad reputation. But in other circumstances, the situation is very different. Men who receive androgen-deprivation therapy for prostate cancer drop their testosterone levels nearly to zero, and when that happens, their cholesterol levels rise. Even within the normal range, men with the lowest testosterone levels tend to have the highest cholesterol levels. And when doctors from the Mayo Clinic reviewed 30 trials of testosterone-replacement therapy, they did not find any overall effect of hormone treatment on cholesterol levels, for good or ill.”17 “Testosterone and the heart.” Harvard Health Publications. March, 2010. (Accessed 7 March 2017.) http://www.health.harvard.edu/heart-health/testosterone-and-the-heart
In any case, the medical community decided that subtlety was not an issue when evaluating the two recent studies on how testosterone therapy affects cognition and the heart, and in multiple editorials they pronounced its uselessness in terms of antiaging. Effectively, the medical community’s summary of the two studies was that testosterone therapy, when used by men over age 65 who have low testosterone levels, offers some health benefits but also poses potential risks. To quote from the editorials, “It improves bone density and anemia in those men. [Really, those are the only benefits they mentioned.] But on the downside, it increases the amount of plaque buildup in coronary arteries while doing nothing to improve cognitive function.” In fact, you didn’t have to go any further than the title of a JAMA editorial to know how they really felt: “Testosterone and Male Aging; Faltering Hope for Rejuvenation.”18 David J. Handelsman. “Testosterone and Male Aging; Faltering Hope for Rejuvenation.” JAMA. 2017;317(7):699-701. http://jamanetwork.com/journals/jama/article-abstract/2603909
The Jokers in the Deck
 There’s a 2015 study published in the European Journal of Endocrinology that almost no one talks about, and yet it’s results should color almost every discussion we have about testosterone–for both men and women. The study found that the use of statins was associated with significantly lower Total T, Free T, and Bioavailable testosterone levels.19 Catherine E de Keyser1, Filipe Valerio de Lima1, Frank H de Jong3, et al. “Use of statins is associated with lower serum total and non-sex hormone-binding globulin-bound testosterone levels in male participants of the Rotterdam Study.” Eur J Endocrinol August 1, 2015 173 155-165. http://www.eje-online.org/content/173/2/155.long In other words, statins decrease your Total T while at the same time increasing the levels of SHBG bound testosterone–absolutely the worst scenario you could have for testosterone. So, why would statin drugs do that? It’s actually quite simple, and I alluded to it earlier.
There’s a 2015 study published in the European Journal of Endocrinology that almost no one talks about, and yet it’s results should color almost every discussion we have about testosterone–for both men and women. The study found that the use of statins was associated with significantly lower Total T, Free T, and Bioavailable testosterone levels.19 Catherine E de Keyser1, Filipe Valerio de Lima1, Frank H de Jong3, et al. “Use of statins is associated with lower serum total and non-sex hormone-binding globulin-bound testosterone levels in male participants of the Rotterdam Study.” Eur J Endocrinol August 1, 2015 173 155-165. http://www.eje-online.org/content/173/2/155.long In other words, statins decrease your Total T while at the same time increasing the levels of SHBG bound testosterone–absolutely the worst scenario you could have for testosterone. So, why would statin drugs do that? It’s actually quite simple, and I alluded to it earlier.
First, because statins decrease cholesterol biosynthesis (that’s why you take them), and because cholesterol is the precursor for testosterone (as we discussed earlier), they reduce testosterone production. This is not theoretical. Studies have shown that statins decrease cholesterol production in testicular Leydig cells.20 Klinefelter GR, Laskey JW & Amann RP. “Statin drugs markedly inhibit testosterone production by rat Leydig cells in vitro: Implications for men.” Reproductive Toxicology. Volume 45, June 2014, Pages 52–58. http://www.sciencedirect.com/science/article/pii/S0890623814000070 In addition, other studies have shown that statins also inhibit enzymes within the testosterone biosynthesis pathway (e.g., 17ß-hydroxysteroid dehydrogenase).21 Smals AG, Weusten JJ, Benraad TJ, Kloppenborg PW. “The HMG-CoA reductase inhibitor simvastatin suppresses human testicular testosterone synthesis in vitro by a selective inhibitory effect on 17-ketosteroid-oxidoreductase enzyme activity.” J Steroid Biochem Mol Biol. 1991 Apr;38(4):465-8. http://www.ncbi.nlm.nih.gov/pubmed/2031860 The net result is that statin drugs produce a lower testosterone level that can lead to symptoms such as a decrease in mood, libido, muscle strength, or bone mineral density.
Why is this so significant? Quite simply it’s because, according to the CDC, the percentage of adults in the United States aged 40 and older taking statin drugs to combat high cholesterol rose from 20 percent to 28 percent between 2003 and 2012–and is continuing to climb.22 Qiuping Gu, Gregg Fonarow. ” Dec. 23, 2014, report, Prescription Cholesterol-lowering Medication Use in Adults Aged 40 and Over: United States, 2003-2012.” CDC NCHS Data Brief. No. 177. December 2014. http://www.cdc.gov/nchs/data/databriefs/db177.pdf Or, to put this in layman’s terms: huge segments of the world’s adult population–both male and female, and especially seniors–are taking medications that actively drive their bioavailable testosterone levels down, down, down.
And that’s why this is the first joker in the deck that we talked about earlier in terms of measuring testosterone. Since statins significantly lower non-SHBG bound testosterone levels, they also significantly lower Bioavailable T levels. So once again, a person with a higher level of Total T, but using statins, would likely have a lower level of Bioavailable T than someone with a lower Total T score but not taking statins.
The Second Joker in the Deck
But every card deck has two jokers. The second one relates to women. Most women in modern society have, at some point in their lives, taken birth control pills. But one study showed that contraceptive use was associated with elevated SHBG levels and reduced bioavailable testosterone, even after discontinuing use. In fact, women that were taking contraceptives at the time of the study had SHBG levels four times higher than those seen in women with no contraceptive exposure.23 Panzer C, Wise S, Fantini G, et al. “Impact of oral contraceptives on sex hormone-binding globulin and androgen levels: a retrospective study in women with sexual dysfunction.” J Sex Med. 2006 Jan;3(1):104-13. http://www.ncbi.nlm.nih.gov/pubmed/16409223 Even women who had stopped taking the Pill for six months were still two times higher in SBHG than the women who had never taken the Pill. In fact, even earlier research has shown that the increases in SHBG levels associated with oral contraceptive use are associated with a concomitant 40–60 percent decrease in free testosterone levels. Keep in mind that lower levels of free testosterone in women are believed to play a major role in weight gain, higher risk of heart attack, as well as sexual problems including decreased sexual desire, decreased arousal, decreased lubrication, and increased sexual pain.
What to Do About Testosterone?
I have to go back to the JAMA editorial headline: “Testosterone and Male Aging; Faltering Hope for Rejuvenation.” Really? This is what you guys came up with based on those studies? What about all of the other rejuvenation benefits that I mentioned earlier–the primary rejuvenation benefits associated with testosterone?
- Increased energy and zest for life.
- Augmented muscle mass and tone, with a concomitant decrease in body fat.
- Increased libido and sexual performance.
Don’t these qualify as rejuvenating benefits? Heck, if nothing else, just testosterone’s indisputably proven benefit to increase muscle mass would be an outstanding rejuvenation benefit. What’s one of the biggest problems associated with aging? Shrinking muscle mass! There’s a reason we refer to “little old men” and “little old women.” And this is not just a cosmetic issue. Shrinking muscle mass in the hips and legs is destabilizing to one’s balance, making an individual more prone to falls. And it’s a double whammy. Not only do shrinking muscles make you less stable and more likely to fall, they provide less cushioning and protection to your bones when you do fall–thus making broken arms, legs, and hips far more likely when you do fall.
So, what’s the bottom line here?
Testosterone is far, far from being a “faltering hope” for rejuvenation. If your level of bioavailable testosterone is low, then getting it back up is essential for rejuvenation.
- Using prescription testosterone supplementation, however, is rarely the best answer–unless there is a specific medical condition preventing you from establishing and maintaining proper levels. Testosterone supplementation is a blunt force tool. Your body normally adjusts testosterone levels in your body hour by hour as the day goes by. Testosterone supplementation lacks that nuance, and while it may address the immediate concern–low Total T–it lacks subtlety. Think of it like using a backhoe on an archeological dig instead of the tools of the trade: trowels and hand brooms. Yes, the backhoe will dig the hole, but it’s also going to damage anything that might be found–as well as miss all of the smaller items that will be hauled away in the giant scoops. It’s the wrong tool for the job–as is testosterone supplementation, in most cases.
- If you’re on statin drugs, you’re going to have to use questionably large amounts of testosterone to raise your blood levels, and you’re still going to have suppressed levels of bioavailable testosterone. You need to find a more body friendly alternative for improving your heart health. And it’s not like the medical community is unified in its support of statin drugs. It’s not.
- The other problem with testosterone supplementation is that if you don’t address the underlying issues, you’re likely to still have problems. For example:
- If your body has high levels of SHBG, then you’re still going to have insufficient levels of bioavailable testosterone even after supplementation.
- If your body has high levels of 5-alpha-reductase and aromatase, then you’re going to end up converting most of that supplemented testosterone into DHT and estrogen, pushing levels of those hormones into the danger zone. (Note: you don’t want to eliminate DHT and estrogen–just keep them under control.)
Fortunately, the use of herbs such as saw palmetto, wild oats, nettles, and Tribulus terrestris can reverse this process in both men and women. Unless you’re saddled with a physiological problem like a tumor on your pituitary gland or non-functioning testes or ovaries, the use of a well-designed testosterone balancing formula can:
- Encourage your body to produce more testosterone naturally.
- Lower levels of 5-alpha-reductase and aromatase so that your body maintains more of the testosterone it produces.
- Hold down SHBG levels, thus increasing bioavailable testosterone levels.
- Inhibit SHBG from binding with testosterone. In fact, this kind of formula can increase bioavailable testosterone levels an astounding 105% on average, as well as repair and rebuild adrenal function!!
- And for men, although we’re not talking about a dedicated prostate formula, the herbs in this formula can slow down the growth of prostate tissue.
For more information on how to optimize your bioavailable testosterone levels, check outThe 30,000 Mile Tune-Up for Men and Women.

References
| ↑1 | Feldman HA, Longcope C, Derby CA, et al. “Age trends in the level of serum testosterone and other hormones in middle-aged men: longitudinal results from the Massachusetts Male Aging Study.” J Clin Endocrinol Metab. 2002 Feb;87(2):589-98. http://www.ncbi.nlm.nih.gov/pubmed/11836290 |
|---|---|
| ↑2 | Wu FC, Tajar A, Pye SR, et al. “Hypothalamic-pituitary-testicular axis disruptions in older men are differentially linked to age and modifiable risk factors: the European Male Aging Study.” J Clin Endocrinol Metab. 2008 Jul;93(7):2737-45. http://www.ncbi.nlm.nih.gov/pubmed/18270261 |
| ↑3 | Harman SM, Metter EJ, Tobin JD, et al; “Baltimore Longitudinal Study of Aging. Longitudinal effects of aging on serum total and free testosterone levels in healthy men. Baltimore Longitudinal Study of Aging.” J Clin Endocrinol Metab. 2001 Feb;86(2):724-31. http://www.ncbi.nlm.nih.gov/pubmed/11158037 |
| ↑4 | Moffat SD, Zonderman AB, Metter EJ, et al. “Longitudinal assessment of serum free testosterone concentration predicts memory performance and cognitive status in elderly men.” J Clin Endocrinol Metab. Nov 2002; 87 (11): 5001-5007. http://www.ncbi.nlm.nih.gov/pubmed/12414864 |
| ↑5 | Morley JE, Kaiser FE, Perry HM, et al. “Longitudinal changes in testosterone, luteinizing hormone, and follicle-stimulating hormone in healthy older men.” Metabolism. Apr 1997 ;46 (4): 410-413. http://www.ncbi.nlm.nih.gov/pubmed/9109845 |
| ↑6 | Araujo AB, O’Donnell AB, Brambilla DJ, et al. “Prevalence and incidence of androgen deficiency in middle-aged and older men: estimates from the Massachusetts Male Aging Study.” J Clin Endocrinol Metab. Dec 2004; 89 (12): 5920-5926. http://www.ncbi.nlm.nih.gov/pubmed/15579737 |
| ↑7 | Rosner W, Auchus RJ, Azziz R, et al. “Position statement: Utility, limitations, and pitfalls in measuring testosterone: an Endocrine Society Position Statement.” J Clin Endocrinol Metab. 2007;92:405-413. http://www.ncbi.nlm.nih.gov/pubmed/17090633 |
| ↑8 | Resnick SM, Matsumoto AM, Stephens-Shields AJ, et al. “Testosterone Treatment and Cognitive Function in Older Men With Low Testosterone and Age-Associated Memory Impairment.” JAMA. 2017;317(7):717-727. http://jamanetwork.com/journals/jama/article-abstract/2603930 |
| ↑9 | Ciocca G, Limoncin E, Carosa E, Di Sante S, et al. “Is Testosterone a Food for the Brain?” Sex Med Rev. 2016 Jan;4(1):15-25. doi: 10.1016/j.sxmr.2015.10.007. http://www.ncbi.nlm.nih.gov/pubmed/27872000 |
| ↑10 | Jung HJ, Shin HS. “Effect of Testosterone Replacement Therapy on Cognitive Performance and Depression in Men with Testosterone Deficiency Syndrome.” World J Mens Health. 2016 Dec;34(3):194-199. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC5209560/ |
| ↑11 | No difference in cognitive impairment seen in men on testosterone treatment.” Healio February 24,2017. (Accessed 5 Mar 2017.) http://www.healio.com/internal-medicine/mens-health/news/online/%7B9b21ef00-301b-4647-bf5f-fd66b03e973a%7D/no-difference-in-cognitive-impairment-seen-in-men-on-testosterone-treatment |
| ↑12 | “Case Closed: Testosterone Does Not Boost Cognition.” ALZFORUM. 24 Feb 2017. (Accessed 5 Mar 2017.) http://www.alzforum.org/news/research-news/case-closed-testosterone-does-not-boost-cognition |
| ↑13 | Wahjoepramono EJ, Asih PR, Aniwiyanti V, Taddei K, Dhaliwal SS, Fuller SJ, Foster J, et al. “The Effects of Testosterone Supplementation on Cognitive Functioning in Older Men.” CNS Neurol Disord Drug Targets. 2016;15(3):337-43. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC5078598/ |
| ↑14 | Budoff MJ, Ellenberg SS, Lewis CE, et al. “Testosterone Treatment and Coronary Artery Plaque Volume in Older Men With Low Testosterone.” JAMA. 2017;317(7):708-716. http://jamanetwork.com/journals/jama/article-abstract/2603929 |
| ↑15 | Marlene Busko. “Atherosclerosis Speeds Up in Older Men on Testosterone: T Trial.” Medscape February 24, 2017. (Accessed 5 Mar 2017.) http://www.medscape.com/viewarticle/876214 |
| ↑16 | Kunal Gururani, , John Jose, and Paul V. George. “Testosterone as a marker of coronary artery disease severity in middle aged males.” Indian Heart Journal, 2016-12-01, Volume 68, Pages S16-S20. http://www.clinicalkey.com/#!/content/playContent/1-s2.0-S0019483216302607 |
| ↑17 | “Testosterone and the heart.” Harvard Health Publications. March, 2010. (Accessed 7 March 2017.) http://www.health.harvard.edu/heart-health/testosterone-and-the-heart |
| ↑18 | David J. Handelsman. “Testosterone and Male Aging; Faltering Hope for Rejuvenation.” JAMA. 2017;317(7):699-701. http://jamanetwork.com/journals/jama/article-abstract/2603909 |
| ↑19 | Catherine E de Keyser1, Filipe Valerio de Lima1, Frank H de Jong3, et al. “Use of statins is associated with lower serum total and non-sex hormone-binding globulin-bound testosterone levels in male participants of the Rotterdam Study.” Eur J Endocrinol August 1, 2015 173 155-165. http://www.eje-online.org/content/173/2/155.long |
| ↑20 | Klinefelter GR, Laskey JW & Amann RP. “Statin drugs markedly inhibit testosterone production by rat Leydig cells in vitro: Implications for men.” Reproductive Toxicology. Volume 45, June 2014, Pages 52–58. http://www.sciencedirect.com/science/article/pii/S0890623814000070 |
| ↑21 | Smals AG, Weusten JJ, Benraad TJ, Kloppenborg PW. “The HMG-CoA reductase inhibitor simvastatin suppresses human testicular testosterone synthesis in vitro by a selective inhibitory effect on 17-ketosteroid-oxidoreductase enzyme activity.” J Steroid Biochem Mol Biol. 1991 Apr;38(4):465-8. http://www.ncbi.nlm.nih.gov/pubmed/2031860 |
| ↑22 | Qiuping Gu, Gregg Fonarow. ” Dec. 23, 2014, report, Prescription Cholesterol-lowering Medication Use in Adults Aged 40 and Over: United States, 2003-2012.” CDC NCHS Data Brief. No. 177. December 2014. http://www.cdc.gov/nchs/data/databriefs/db177.pdf |
| ↑23 | Panzer C, Wise S, Fantini G, et al. “Impact of oral contraceptives on sex hormone-binding globulin and androgen levels: a retrospective study in women with sexual dysfunction.” J Sex Med. 2006 Jan;3(1):104-13. http://www.ncbi.nlm.nih.gov/pubmed/16409223 |








Just one more thing to add to
Just one more thing to add to the list of serious side effects from statin drugs. That list seems to grow & grow.
A number of years ago I begged my daughter to NOT take them. I know I would not.
GET HER OFF OF STATINS AND
GET HER OFF OF STATINS AND GET HER ON CITRUS BERGAMOT, A NATURAL FRUIT, WHICH WILL NOT ONLY LOWER BAD CHOLESTEROL, TRIGLYCERIDES, ETC., BUT ALSO RAISE THE GOOD CHOLESEROL, WHICH STATINS DO NOT DO!!!
Mr. Barron,
Mr. Barron,
Your TESTOSTERONE article is excellent. How about a ‘follow up’ article concerning the two types of Testosterone tests; the “older” ANALOG type and the FORMULA type. They both show different amounts and ranges of existing Total and Free testosterone; which, in your opinion, is the more accurate type of test and what do they involve?
Very Respectfully,
Dr. Robert Bolmarcich
PH.D. M.E.
As Jon says in the article,
As Jon says in the article, “Liquid chromatography tandem mass spectrometry (LC-MS/MS) has become the method of choice for steroid hormone measurements. But even here, things are not necessarily straightforward. Yes, LC-MS/MS requires only small sample volumes and offers fast analysis times, but it is much more complex, and its accuracy is dependent in the skill of the lab tech in preparing the samples for testing and thus can vary notably from test to test.” http://www.ncbi.nlm.nih.gov/pubmed/17090633
Very helpful article. As a 61
Very helpful article. As a 61 year old male I found that by taking one-quarter of a 1 mg pill of Arimidex (anastrozole) every third day I have been able to lose weight, put on muscle mass, and have more energy. This is a prescription drug but can be purchased legally without a prescription in liquid form. It is an aromatase inhibitor (AI) which stops the aromatase enzyme from converting testosterone into estrogen, thereby freeing up testosterone. This drug has no side effects unless you take too much and drop your estrogen level too low. I learned this from the world of body building where they use various aromatase inhibitors to free up more testosterone. Some physicians are well aware of this and work with it just fine. Yet a man needs to be careful not to take too much. A man will know if he takes too much as he will stop having nighttime erections. If you take the right amount your nighttime erections will be like when you were a young man. Thus a man has a very easy way to tell if he has dosed right. Take too much and you can also get moody, and it takes about a month for it to wear off. Thus it is best to find a doctor who understands hormonal therapy so you can do this under a doctor’s guidance. I also take Jon Barron’s Men’s Formula, 3 droppers a day. I also follow Barron’s Baseline program. I have lost 105 pounds, cured my diabetes as in got my blood sugar down from 300 to under 100 most of the time, and got my blood pressure down from the 145/ 85 range down to the 105/65 range with a pulse of average 65 bpm. No insulin or other drugs except the very low dose of Arimidex as fat makes estrogen. I have 15 more pounds to go. I also use a rebounder for short but hard interval exercise. This is just my personal experience. Ask your trusted heath care practitioner before you try it.
I saw testosterone was made
I saw testosterone was made from cholesterol, and though not reading every word, then saw the paragraph,
“There’s a 2015 study published in the European Journal of Endocrinology that almost no one talks about, and yet it’s results should color almost every discussion we have about testosterone–for both men and women. The study found that the use of statins was associated with significantly lower Total T, Free T, and Bioavailable testosterone levels.19 In other words, statins decrease your Total T while at the same time increasing the levels of SHBG bound testosterone–absolutely the worst scenario you could have for testosterone. So, why would statin drugs do that? It’s actually quite simple, and I alluded to it earlier.”
Before seeing this paragraph, I wondered does niacin do the same thing? Maybe I should read more thoroughly, as you may have mentioned this.
Although niacin can lower
Although niacin can lower cholesterol, it’s not in the same league as statin drugs, which are much, much stronger. Using niacin, you would never have an issue about pushing cholesterol numbers so low as to be problematic.
Dear Jon, thank you for your
Dear Jon, thank you for your article.
Could you please elaborate more about interaction between testosterone and prostate BPH? I used to enhance my testosterone levels taking tribulus terrestris. It helped managing my weight and sustaining a healthy sexual life.
However, since discovering that I have BPH and PSA near 10, I stopped taking tribulus, worried that it had caused BPH. I’d like to add that I’ve had two MRAs within two years and the prostate looks normal, albeit enlarged.
I’m currently taking some of the ingredients of your formula, like saw palmetto and ginseng, managing my BPH successfully, but I’m reluctant to mix with sexual enhancers to prevent side effects of testosterone, if any.
Could you please advise? Many thanks in advance.
Vincenzo
For obvious legal reasons, we
For obvious legal reasons, we cannot diagnose or prescribe for specific medical conditions—merely, provide information. With that in mind…
It is highly unlikely that Tribulus caused your BPH. In fact, studies would indicate just the opposite. http://www.ncbi.nlm.nih.gov/pubmed/22177370. You might also find the following article informative. https://jonbarron.org/anti-aging/barron-report-remedies-hormonal-changes-1
Similar to the question
Similar to the question regarding niacin, does Red Rice Yeast adversely affect bioavailability of T.? I understand that this ancient yeast product has something in common chemically with some statins, and is recommended for reduction of bad cholesterol as an herbal “stand in” for statins… THANKS!