Last newsletter, we examined the anatomy of the urinary system. Today, we’re going to examine the urinary system’s functions — focusing almost entirely on how your kidneys (and more specifically, the kidneys’ nephrons) actually filter and balance your blood. Understanding how this works, and how you can prevent and reverse damage to the process and even assist it, is fundamental to maintaining optimum health. We’ll conclude by exploring what your doctor learns about you when examining the results of your urinalysis. Wouldn’t it be nice to actually know what your doctor is talking about when she makes recommendations to you based on the results of your test?
Quick review of the anatomy of the urinary system
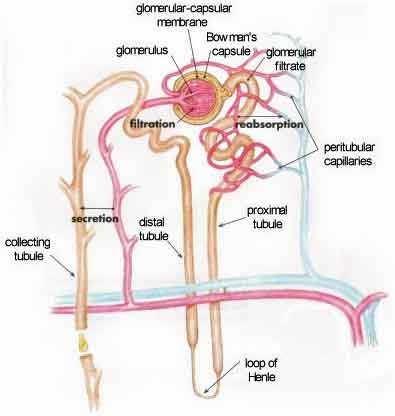
As we discussed previously, water, waste, and in fact virtually everything other than red and white blood cells are pulled out of the blood in the balled mass of arterioles known as the glomerulus, located at the front end of the nephron. All of this “waste” material then passes into the renal tubule portion of the nephron for “fine tuning.” Keep in mind, that at this point, what we’re referring to as waste contains virtually everything including the kitchen sink. If your body could not reclaim most of these elements, since many are essential for life, you would quickly die. That’s why that as this pre-urine makes its way through the tubules of the nephron, it is fine tuned, with a bunch of things, including the water, that were previously extracted being put back into the bloodstream, as required by your body. In addition, some other things, such as medications, are pulled out in the tubules, as they are determined to be unnecessary during the process of fine tuning.
To summarize: The primary purpose of kidney filtration is to balance out bio-chemicals in the bloodstream — to achieve homeostasis. Excretion of toxins is a byproduct of this function. The stages involved in the process are glomerular filtration, tubular reabsorption, and tubular secretion. Let’s now explore these elements in detail.
Kidney homeostasis
As we’ve said several times, the primary function of the kidneys is to maintain homeostasis. Excretion is a byproduct of that homeostasis. The general mechanisms used by the kidneys for maintaining homeostasis include:
- Regulation of water volume, blood volume, and interstitial fluid volume. One of the first warning signs that your kidneys are not functioning properly is water retention, or edema — as evidenced by swelling in your ankles and legs.
- Reabsorption of required substances that were removed in the glomerulus. This included ions such as sodium, calcium, and bicarbonate; amino acids such as glutamate; carbohydrates such as glucose, and water.
- Excretion of excess substances. These are the same substances that we just listed as possible for reabsorption. It’s all a question of what and how much your body needs to maintain its bio-chemical balance.
- Excretion of toxic substances — primarily uric acid, creatinine (not to be confused with creatine), and lymphatic waste.
- Regulation of body pH.
- Regulation of normal blood pressure — primarily by regulating water and sodium levels in the blood.
To summarize: when excess water, sodium ions, calcium ions, potassium ions, and so on are present, the excess quickly passes out in the urine. On the other hand, the kidneys step up their reclamation of these same substances when they are present in the blood in less-than-normal amounts. Thus the kidney continuously regulates the chemical composition of the blood within narrow limits. The kidney is one of the major homeostatic devices of the body. And the first step in effecting this homeostasis is glomerular filtration.
Filtration in the nephron
In our last issue when we discussed the anatomy of the kidney, we identified areas in the kidney such as the medulla, cortex, and papillary ducts. But these are not functional units; they are merely defined regions useful for identification. In the kidney, the nephron is “the” functioning unit. As we’ve already mentioned, filtration in the nephron, in its simplest terms, is a three step process.
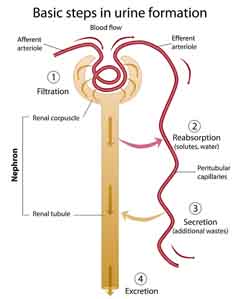 First, pressure pushes fluid and solutes (the glomerular filtrate) through microscopic holes in the glomerular capillaries. This pressure results primarily from the fact that the afferent arteriole entering the glomerulus is larger than the efferent arteriole that leaves it. Think of it like running a river through a narrow gorge. You get rapids and increased pressure. In other words, the pressure pushing into the renal corpuscle from the afferent arteriole is greater than the smaller efferent arterioles can handle. It is this pressure that “pushes” almost everything except the red and white blood cells and large proteins across the walls of the glomerular capillaries into the collecting system of the glomerulus. As a result, the kidneys wipe the blood clean — in effect, creating “a clean slate.” Unfortunately, many of those things filtered out are required for life, but that’s where homeostasis kicks in. Regulated by signals from other parts of the body, as the filtrate moves through the tubules of the nephron, necessary components in precise amounts are reabsorbed by the peritubular capillaries back into the system.
First, pressure pushes fluid and solutes (the glomerular filtrate) through microscopic holes in the glomerular capillaries. This pressure results primarily from the fact that the afferent arteriole entering the glomerulus is larger than the efferent arteriole that leaves it. Think of it like running a river through a narrow gorge. You get rapids and increased pressure. In other words, the pressure pushing into the renal corpuscle from the afferent arteriole is greater than the smaller efferent arterioles can handle. It is this pressure that “pushes” almost everything except the red and white blood cells and large proteins across the walls of the glomerular capillaries into the collecting system of the glomerulus. As a result, the kidneys wipe the blood clean — in effect, creating “a clean slate.” Unfortunately, many of those things filtered out are required for life, but that’s where homeostasis kicks in. Regulated by signals from other parts of the body, as the filtrate moves through the tubules of the nephron, necessary components in precise amounts are reabsorbed by the peritubular capillaries back into the system.
Tubular reabsorption, which takes place throughout the convoluted tubules and the loop of Henle, reclaims both water and important solutes from the filtrate and puts them back into the bloodstream and is the second stop in the process. This is accomplished by moving solutes back and forth as needed across the walls of the tubules into the peritubular capillaries that feed them — or from the peritubular capillaries back into the tubules as required. When wastes are pushed back into the tubules for disposal, that is called tubular secretion, and that is the third step in the filtration process. Whatever is left is excreted.
If you’re having a hard time following things at this stage, don’t worry. We’re now going to go one more level down in detail, and in this case, more detail actually makes things more understandable. Let’s break our three step process down by location in the nephron and see exactly how things work at each location. We’re going to look at what happens in five specific areas/locations of the nephron:
- The glomerulus, as contained in the capsule of Bowman.
- The proximal convoluted tubule, which receives the filtrate from the glomerulus.
- The descending loop of Henle.
- The ascending loop of Henle.
- The distal convoluted tubule
The glomerulus
As we mentioned earlier, the driving force in the glomerulus, all puns intended, is glomerular filtration pressure. In order to understand this, we need to take a little detour and discuss blood pressure — the regulation of which is one of the primary functions of the kidney.
 Blood pressure is the pressure exerted by circulating blood upon the walls of blood vessels. It is measured in terms of millimeters of mercury (mmHg). What does this mean? Although not as common as they once were, mercury based sphygmomanometers were at one time the only way to measure blood pressure based on how far the pressure in your blood could push mercury up a tube — like an old fashioned barometer. And that distance was measured in millimeters. The two numbers you get when you take your blood pressure, 120 over 80, for example, refer to the two distances your blood pressure could push mercury up a tube, depending on whether your heart was beating (the higher number) or at rest between beats (the lower number). Which brings us back to glomerular filtration pressure.
Blood pressure is the pressure exerted by circulating blood upon the walls of blood vessels. It is measured in terms of millimeters of mercury (mmHg). What does this mean? Although not as common as they once were, mercury based sphygmomanometers were at one time the only way to measure blood pressure based on how far the pressure in your blood could push mercury up a tube — like an old fashioned barometer. And that distance was measured in millimeters. The two numbers you get when you take your blood pressure, 120 over 80, for example, refer to the two distances your blood pressure could push mercury up a tube, depending on whether your heart was beating (the higher number) or at rest between beats (the lower number). Which brings us back to glomerular filtration pressure.
Normal blood pressure in the afferent arteriole of the nephron is about 55 mmHG– about half of what it is in the rest of your circulatory system. Make sense so far? The filtrate which has already been pulled out of the glomerular capillaries but that is still sitting in glomerulus capsule surrounding the capillaries exerts a back pressure of about 15 mmHg in the opposite direction. And then there is the osmotic back pressure produced by the proteins and other solids in the blood, which amounts to about 30 mmHg pushing back against the afferent arteriole pressure. Or to put it another way, while much of the water in the blood crosses the glomerular capillaries into the glomerular capsule, most of the proteins do not. These proteins then exert an increasing osmotic “pull” on the water in the plasma filtrate surrounding the capillaries. The net filtration pressure then is 55 mmHg — 15 mmHg — 30 mmHg = 10 mm Hg. In normal circumstances, that 10 mmHG of filtration pressure in the nephrons remains pretty constant. And it is this net filtration pressure that pushes filtrate through the kidneys. It should be noted, however, that both high and low blood pressure affect the glomerular filtration rate in opposite directions, but both with negative consequences. We’ll talk more about both high and low blood pressure and the kidneys later. For now, though, all you need to remember is that blood pressure drives filtration in the kidneys and that both high and low blood pressure present problems for the kidneys — but they have tools for compensating.
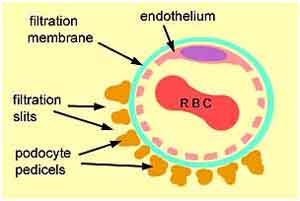 Now that we understand the pressure that forces filtrate across the glomerular capillaries, we need to understand what actually does the filtering. What regulates what passes into the filtrate and what stays in the blood — at least in the glomerulus? And for that, we return to our discussion of the anatomy of the capillaries/arterioles in the glomerulus. As you may remember, they contain different sized filters — the endothelium, the basement membrane, and the slit membrane — that filter out large proteins. After all, we don’t want blood cells (red or white) in the urine. We don’t want complex proteins such as albumin to go out either. Pretty much everything else, however, is allowed to pass out of the blood along with the filtrate through the walls of the capillaries and into the surrounding capsule. This means that a whole range of bio-chemicals including glucose, amino acids, small proteins, waste molecules (like urea), Na, K, Cl, and HCO3 ions — not to mention a ton of water — travel out with the filtrate to be pulled back into the bloodstream as needed a little further along in the nephron.
Now that we understand the pressure that forces filtrate across the glomerular capillaries, we need to understand what actually does the filtering. What regulates what passes into the filtrate and what stays in the blood — at least in the glomerulus? And for that, we return to our discussion of the anatomy of the capillaries/arterioles in the glomerulus. As you may remember, they contain different sized filters — the endothelium, the basement membrane, and the slit membrane — that filter out large proteins. After all, we don’t want blood cells (red or white) in the urine. We don’t want complex proteins such as albumin to go out either. Pretty much everything else, however, is allowed to pass out of the blood along with the filtrate through the walls of the capillaries and into the surrounding capsule. This means that a whole range of bio-chemicals including glucose, amino acids, small proteins, waste molecules (like urea), Na, K, Cl, and HCO3 ions — not to mention a ton of water — travel out with the filtrate to be pulled back into the bloodstream as needed a little further along in the nephron.
Tubular reabsorption
Most of the water in the tubules must be reabsorbed before it passes out to the bladder to prevent dehydration, which would occur within hours. Your kidneys literally extract some 180 liters/quarts of water a day. If it didn’t put almost all of it back, you’d dry up like a prune in a matter of hours. Also, in addition to water, most of the solutes (glucose, amino acids, sodium, chloride, potassium, phosphate, and bicarbonate) are both actively and passively reabsorbed in the tubules.
How is this accomplished?
A large chunk of the work is done in the proximal convoluted tubule located immediately after the glomerulus. Some of this reabsorption takes place automatically, and some is the result of chemical signals — particularly in terms of acid and alkaline levels.
Ninety percent of the reabsorption is passive (obligatory) water reabsorption. It occurs by osmosis, primarily in the proximal convoluted tubule (although some also occurs in the descending limb of the loop of Henle, and the distal convoluted tubule). The proximal tubule also regulates the pH of the filtrate by exchanging acidic hydrogen ions in the peritubular capillaries surrounding the tubule for alkaline bicarbonate ions in the filtrate until a state of acid/alkaline balance is attained. Of course, if there are too few bicarbonate ions in the filtrate to balance out the hydrogen ions present in the surrounding capillaries, then your blood will start tending toward an unhealthy acid state. And since your blood can’t tolerate much change in its pH, it will start offloading the excess acidity into all of the soft tissue and muscle that it feeds.
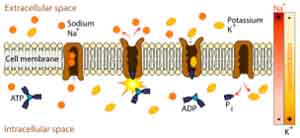
The reabsorption is driven by the same sodium/potassium pump mechanism that we explored when talking about absorption in the small intestine.
So exactly what is reabsorbed in the proximal tube? (Remember, reabsorption continues as the filtrate continues its trip through the nephron.)
| Substance | % of filtrate reabsorbed in the proximal convoluted tubule |
| Salt and water | Approximately 66% |
| Glucose (sugar) | 100% — unless there’s a problem |
| Amino acids | 100% — unless there’s a problem |
| Potassium | Approximately 66% |
| Urea | Approximately 50% |
| Phosphate (regulated by parathyroid hormone) | Approximately 80% |
Tubular secretion
Not all movement in the proximal tubule is “out.” Some waste substances are secreted from the tissue and capillaries surrounding the tissue “into” the tubule. Many types of medication, for example, make their way out of the body by secretion into the proximal tubule. This includes furosemide (a diuretic), methotrexate (a cancer drug), the antibiotics penicillin, gentamicin, and tetracycline, and digoxin (the heart medication) to name just a few. In addition, a large portion of the creatinine, produced as a byproduct of muscle activity, passes into the urine in the proximal tubule.
And finally, most of the ammonium that is excreted in the urine is formed in the proximal tubule as a result of the breakdown of glutamine to alpha-ketoglutarate.
The loop of Henle
As with the proximal tubule, the processes of both reabsorption and secretion continue in the loop of Henle. As shown in the table above, approximately 2/3 of the water in your urine is reabsorbed in the proximal tube. Almost all the rest of it is reabsorbed in the loop of Henle. In truth, only a very, very tiny percentage of the water (1-2 quarts/liters) that is passed out in the glomerulus actually makes its way to your bladder.
Also, it is in the loop of Henle, particularly in the ascending loop that the sodium, potassium, and chloride ions are reabsorbed into the body.
The distal convoluted tubule
This is the last stop for any adjustments to your urine. After passing through this second convoluted tubule, your urine enters the collection tubules and flows on out of the kidney and your body. This final ten percent of water reabsorption, which takes place in the nephron’s distal tubule, is not automatic but happens in response to circumstances and triggers from all over the body. In other words, it is not a passive process, as in the proximal tubule, but is now controlled and aided by hydration signals from the body — specifically, antidiuretic hormone (ADH), which comes from the brain, and aldosterone, which comes from the adrenals. ADH is secreted by the posterior pituitary to act on the principal cells of the distal convoluted tubules to increase their uptake of water. Aldosterone likewise signals the principal cells to increase their uptake of water as well as their uptake of sodium.
The walls of the distal tubules also represent the primary location in the body of the protein arginine vasopressin receptor 2, which responds, as its name suggests, to the hormone arginine vasopressin by stimulating mechanisms in the distal tubule that concentrate the urine and maintain water homeostasis. Vasopressin is produced in the hypothalamus and stored in the pituitary to be released as needed to stimulate more reabsorption of water in the kidneys — according to signals received in the brain.
Again, this makes the distal tubule the final arbiter in regulating urine concentration and water homeostasis in the body.
It is also in the distal convoluted tubule that your body makes its final pH adjustments for your bloodstream by shuttling alkaline bicarbonate and acidic H+ hydrogen protons either into or out of the filtrate as required to regulate the pH in the blood in the peritubular capillaries. And finally, calcium blood levels are regulated in the distal tubule, as calcium is reabsorbed into the body in response to parathyroid hormone secretions coming from your neck.
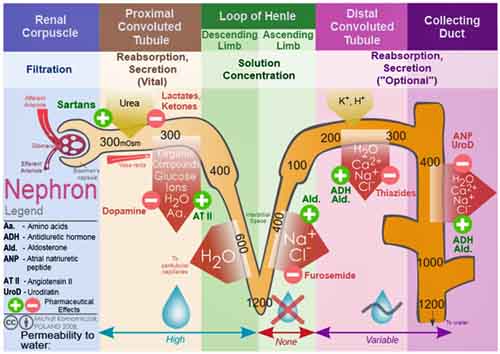
The following chart summarizes what flows from the bloodstream to the nephron and back again, and exactly where in the nephron the exchange takes place.
Micro-anatomical areas of the nephron and low blood pressure
There is one other thing that the kidneys/nephrons do that needs to be mentioned. The nephrons not only process blood that flows through them; they also monitor it. And if they sense that blood pressure is low — let’s say as the result of a severe injury — they have the ability to respond.
The juxtaglomerular apparatus is a microscopic structure that surrounds the afferent arteriole at the point where it enters the glomerulus. It consists of juxtaglomerular cells, which secrete renin if they detect low sodium levels or low blood volume in the blood passing through the afferent arteriole. Renin is an enzyme that controls the activation of the hormone angiotensin, which stimulates the adrenal glands to produce aldosterone. Aldosterone tells the kidneys to retain sodium and water, thus pushing blood pressure up.
The macula densa is an area of specialized cells lining the wall of the distal convoluted tubule at the point where it is closest to the glomerulus as it returns from the ascending loop of Henle. The cells of the macula densa are sensitive to the concentration of sodium chloride in the tubule. If the macula densa cells sense low sodium levels or low blood volume, they trigger the increase of blood flow through the afferent arteriole thus pushing filtration rates and pressure back towards normal. And they increase the release of renin from the juxtaglomerular cells, which further pushes up blood pressure.
The end result
The blood flow to the kidneys is extraordinarily large. Together, the two kidneys receive 20% of the total blood flow in your body at any point in time. Keep in mind, that’s the same amount as the brain gets. Between brain and kidneys, that’s 40% of your blood flow. And if you think about it, proportionally, it’s actually much higher than the brain since your kidneys, together, only weigh about ¼ as much as your brain. In other words, your kidneys received four times as much blood flow as your brain per unit of tissue. Effectively, your kidneys receive more of your blood and bodily fluids than any other organ in your body.
How much?
About 125 ml of water and dissolved substances are filtered out of the blood each and every minute of each and every day. That works out to some 7500 ml per hours, or about 180 liters or 47 gallons per day; but, as we discussed earlier, 99% of that is reabsorbed back into your body — otherwise, you would dry up like a prune in a matter of hours and blow away like dust in the wind. With that in mind, let’s take a look at what substances are actually filtered out of your blood every day, how much is reabsorbed, and how much is excreted in the urine. And keep in mind that we actually only have about 4-6 quarts/liters of blood in total, which makes the numbers below pretty astounding)
| Substance | Filtered (enters glomerular capsule per day) | Reabsorbed (returned to blood per day) | Urine (excreted per day) |
| Water | 180 liters
About 47 gallons a day! |
178-179 liters | 1-2 liters (thus the 8 glasses of water you need to drink every day to replace what’s lost) |
| Proteins (small) | 2.0 g | 1.9 g | 0.1 g |
| Sodium ions (Na+) | 579 g | 575 g | 2-4 g (a healthy person can handle up to about 4.2 g of sodium per day in their diet) |
| Chloride ions (Cl-) | 640 g | 633.7 g | 6.3 g |
| Bicarbonate ions (HCO3-) | 275 g | 275 g | 0.03 g |
| Glucose | 162 g | 162 g | 0 g (any sugar in the urine is abnormal) |
| Urea | 54 g | 24 g | 30 g |
| Potassium (K+) | 29.6 g | 29.6 g | 2.0 g |
| Uric acid | 8.5 g | 7.7 g | 0.8 g |
| Creatinine (breakdown product of muscle metabolism) | 1.8 g | 0 g | 1.7 g |
A consideration
When considering how much filtering is actually being done by your nephrons, it’s worth putting it in perspective to fully appreciate what they do.
- You only have 1- 1½ gallon of blood, and yet your kidneys filter approximately 1700 liters (449 gallons) of blood a day. In other words, your kidneys filter your entire blood supply over and over again some 400 times a day.
- They remove upwards of 47 gallons of water from that blood every day and then return some 46 gallons of that same water back to your blood.
- Your kidneys are each about the size of a small fist.
- The functioning unit in the kidney is the nephron, and each nephron is 3 cm or about 1inch long — but also extremely narrow, especially in the descending loop of Henle.
- Each kidney contains one million nephrons crammed into that fist sized space (a testament to how narrow they actually are).
- That means because the tubules are so narrow and move such a massive amount of fluid and solute, they are extremely easy to clog with stones and sludge, thus shutting down large areas of the kidney over time (which we will talk about in our next newsletter).
For a review of this filtration process, check out:
Urine testing
If you’ve hung with us so far, we get to the first of the payoffs. Now that we have an understanding of how the kidneys work, we have a basis to understand what doctors look for when they do a urinalysis — to understand what those results mean for our health. Let’s take a look.
Urine’s physical characteristics
The first thing a doctor checks for when examining your urine are its obvious physical characteristics: color, clarity, odor, and in the good old days…taste. The urine of a diabetic actually tastes sweet because of the glucose in it. Before we had scientific testing for sugar in the urine, you could taste the sugar in urine long before you could smell it. Alas, physicians just don’t have that kind of dedication anymore.
Color
Urine is normally pale to dark yellow in color. Keeping in mind that many foods, supplements (B vitamins, for example), and medications can affect its color, there are still things that can be readily perceived. Urine with no color may be a cause for concern as it indicates dilute urine where lots of water is being excreted. Possible causes include long-term kidney disease or uncontrolled diabetes. At the other end of the spectrum, dark yellow urine can be caused by dehydration or fever. It’s also common in the “first morning” urine. And two colors that you absolutely don’t want to see are red and brown. These colors mean that there is most likely blood in the urine.
Clarity
Healthy urine, based on our observation of how the nephrons work, is obviously clear, or at worst, slightly cloudy. Cloudy or turbid urine indicates a problem as it can be caused by pus from an infection, blood, sperm, bacteria, yeast, calcium crystals, mucus, or even a parasite infection. None of which you want in your urine.
Odor
And healthy urine has what is most often described as a “nutty” smell. And as most of us are aware, some foods (such as asparagus), certain vitamins or antioxidants, and even antibiotics such as penicillin can change the fragrance. But the one smell you absolutely don’t want is a sweet, fruity odor, which is a common signal for uncontrolled diabetes. And a distinctly “foul” odor is a sign of a urinary tract infection.
General measurements
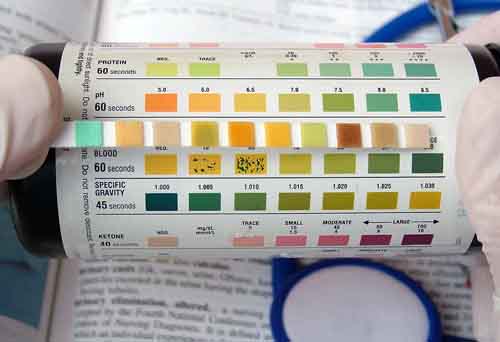
The two general measurements that your physician will look at in your urinalysis are specific gravity and pH.
Specific gravity
Specific gravity is the ratio of the density of a substance compared to water. It shows how concentrated particles are in your urine. The specific gravity of water is 1, so the closer the number comes to 1, the fewer particles will be found in it. Again, based on what we know about the formation of urine, we would expect that number to be very, very close to water itself…and it is. The normal specific gravity of urine is 1.010-1.020. Why that sounds so close to fresh water to be good enough to drink — or not! Obviously, urine’s specific gravity can’t go lower than water since it’s essentially water plus. Although, if it drops lower than 1.005, it means that your urine is too dilute, which may be caused by drinking too much water, severe kidney disease, or the use of diuretics. On the other hand, a high specific gravity means very concentrated urine, which is a sign of dehydration. This can be caused by not drinking enough fluid, loss of too much fluid from excessive vomiting, sweating, or diarrhea, or from substances such as sugar or protein in the urine. Knowing the urine concentration also helps doctors decide if the urine specimen they are evaluating is the best one to detect a particular substance. For example, if they are looking for very small amounts of protein, a concentrated morning urine specimen would be the best sample.
pH
The other general number that often appears in a urinalysis is pH. Normal healthy urine pH is slightly acidic, around 5.0 — 6.0, but on any given day, urine pH can range from 4.6-8.0. Keep in mind that certain foods such as citrus fruit, dairy products, and cola drinks, not to mention medicines such as antacids can affect urine pH. An abnormal reading on a single test doesn’t necessarily mean much. An abnormal number that appears consistently over several tests probably does. A high pH, or excessive alkaline reading, can be caused by severe vomiting, a kidney disease, some urinary tract infections, and asthma. A low pH, or acidic reading, may be caused by severe lung disease (which reduces the body’s ability to clear CO2), uncontrolled diabetes, aspirin overdose, severe diarrhea, dehydration, starvation, or heavy consumption of alcohol.
Some people who actively monitor their pH levels obsess over urine pH levels, trying to raise them solidly into alkaline territory. That’s probably not a good idea as urinary tract infections find an alkaline environment more amenable than an acid one. On the other hand, you absolutely and most definitely want an alkaline pH in your blood, saliva, and soft tissue. Just don’t get carried away trying to force your urine into an alkaline state. Not everything acid in the body is bad. Think stomach acid…and now urine.
Canaries in the coal mine
Beyond its general characteristics, your doctor will look for the presence of specific substances, which can signal serious problems if they are found. This includes sugar, protein, ketones, red or white blood cells, crystals, bacteria, yeast cells, parasites, urinary casts, and endothelial squamous cells from the kidneys.
Glucose
First and foremost is glucose, or sugar. As we’ve already learned, 100% of the glucose in your urine should be reabsorbed in the tubules of your nephrons. There should be absolutely no “detectable” sugar in your urine — unless you’re pregnant or perhaps receiving a glucose IV while in the hospital. Other than those exceptions, it’s a problem. Glucose usually spills into the urine when the blood sugar level exceeds 200 mg/dl. When glucose is present in the urine, it’s called glucosuria. Its primary cause is obviously diabetes — an excessively high concentration of sugar in the blood. Another possibility, although much rarer, is an intrinsic problem with the ability of the kidneys to reabsorb sugar in the tubules of the nephron, independent of sugar levels in the blood. Problems in the adrenal glands and/or the liver can also put sugar in the urine. Even certain types of brain injury, believe it or not, can cause sugar to appear in the urine. Any detection of sugar in the urine calls for follow up testing.
Protein – albumin
Also, as we know, there should be no large proteins in your urine. The filtering mechanism, if functioning properly, doesn’t allow it. Specifically, urinalysis measures the amount of albumin protein in the urine. While low levels of albumin “usually” aren’t a cause for concern, the presence of protein at any notable level is potentially a sign of serious problems, including:
- Kidney damage
- Infection
- Glomerulonephritis (inflammation of the renal capillaries)
- Diabetes
- High blood pressure
- Cancer
- Lupus
- Heart failure
- And even mercury poisoning
Note: trace amounts of protein can be normal in athletic individuals as the result of heavy workouts. Protein is also sometimes seen in male urine due to leakage from the prostate.
 Crystals
Crystals
Large amounts of crystals, or certain types of crystals, can mean kidney stones, damaged kidneys, or problems with metabolism. Some medicines and some types of urinary tract infections can also increase the number of crystals in the urine. And in almost all cases, the presence of any crystals in the urine is an indication that sludge has formed in the kidneys. The sludge may not have formed into full-fledged stones, which is where medical doctors take note, but the presence of sludge of any type in your nephrons is a serious concern, and it is a signal that you should take note. (We’ll talk more about sludge in the next part of our series on the urinary tract.)
Ketones
Ketones are produced as by-products when fatty acids are broken down for energy in the liver and kidneys. There should be no “detectable” ketones in your urine. Their presence can be a sign of uncontrolled diabetes. (By now, you probably should have come to the conclusion that if you have sugar, proteins, and ketones in your urine, you pretty much have diabetes.) However, ketones can also start appearing in the urine after severe exercise or when the body starts consuming itself as the result of low-carbohydrate diets, eating disorders, or starvation. Promoters of low-carb diets such as the Atkins diet say that the presence of ketones is actually a good thing. Pretty much everyone else says it’s not.
Blood cells
Red blood cells in the urine may be caused by many of the same things that cause protein to be found in the urine: kidney or bladder injury, kidney stones, a urinary tract infection, inflammation of the kidneys (glomerulonephritis), a kidney or bladder tumor, or lupus. There are always a few white blood cells (pus) in the urine; it only signals a problem when the number of white blood cells increases significantly. The increase may be caused by a urinary tract infection, bladder tumor, inflammation of the kidneys, lupus, a vaginal infection, or an infection under the foreskin of the penis.
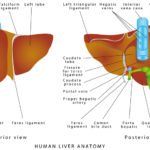
Bilirubin
Bilirubin is a product of red blood cell breakdown. Normally, bilirubin is carried in the blood and passes into your liver, where it’s removed and becomes part of bile. Bilirubin in your urine may indicate liver damage or disease. Urobilinogen is formed in the intestine from bilirubin, and a portion of it is absorbed back into the bloodstream. It is normally present in urine in low concentrations. Positive test results at higher levels help detect liver diseases such as hepatitis and cirrhosis and conditions associated with increased red blood cell destruction, such as hemolytic anemia. When urine urobilinogen is low or absent in a patient with urine bilirubin and/or signs of liver dysfunction, it can indicate the presence of liver, gallbladder, or bile duct obstruction.
Casts
Depending on the type, the presence of casts in the urine can indicate inflammation or damage to the tiny tubes in the kidneys, poor blood supply to the kidneys, metal poisoning (such as lead or mercury), heart failure, or a bacterial infection. Casts are cylindrical particles sometimes found in urine that are formed from coagulated protein secreted by kidney cells. They form in the distal convoluted tubules and usually take the shape of the tubule (hence the name). Under the microscope, they often mimic the shape of a “hot dog,” and in healthy people they appear nearly clear.
Bacteria, yeast, and parasites
Bacteria in the urine mean a urinary tract infection. Yeast cells or parasites (such as the parasite that causes trichomoniasis) can also mean an infection of the urinary tract.
Epithelial cells
Normally, a few epithelial cells from the bladder or from the external urethra (squamous epithelial cells) can be found in the urine sediment. Cells from the kidney (kidney cells) are less common. In urinary tract conditions such as infections, inflammation, and malignancies, more epithelial cells are present. For example, a bladder infection may result in large numbers of transitional epithelial cells in urine sediment. Epithelial cells are usually reported as “few,” “moderate,” or “many.”
Conclusion
Urinalysis is used as a screening and/or diagnostic tool because it can help detect substances or cellular material in the urine associated with different metabolic and kidney disorders — conditions which caused the nephrons to fail in their job. It is ordered widely and routinely to detect any abnormalities that require follow up. However, it does not provide a definitive diagnosis. Depending on the reason your doctor recommended the test in the first place, abnormal results may or may not require follow-up. Your doctor may need to evaluate the results along with those of other tests, or additional tests may be necessary to determine next steps. Remember, even the medications your doctor has previously given you may produce abnormal, but expected, results and are not a cause for concern. Your doctor will know this…one hopes.
In summary, if you are otherwise healthy and have no signs or symptoms or illness, results slightly above or below normal on a urinalysis may not be a cause for concern and follow-up may not be needed. However, if you’ve already been diagnosed with kidney or urinary tract disease and undergoing treatment, elevated levels may indicate a need to alter your treatment plan.

That’s it for now. In the final part of our series, we’ll take on the conditions that can compromise kidney function and how to prevent and possibly even reverse them — and an unusual therapy based on urine that some alternative healers swear by.





wonderful explanation indeed.
wonderful explanation indeed. thank you very much for the basic knowledge u hve provided. thanks lot. please keep it up this self-education tools of all imp organs, which is most important for preventing or to get cured any disease.
venkatesh
This newsletter is very
This newsletter is very informative, thank you. It doesnt really answer my question as to why I get frequent cystitis. Maybe your next news letter will help.
Actually, Jon’s first
Actually, Jon’s first newsletter in the Urinary System series covers cystitis and the urinary tract infections that often are its cause in some detail. http://www.jonbarron.org/what-causes-kidney-stones/anatomy-urinary-system-newsletter
"Waterfall D Mannose has the
“Waterfall D Mannose has the ability to attach to bacteria and prevent the bacteria from attaching to your bladder wall. When you stop the bacteria from attaching, you stop bladder infection symptoms, because when bacteria can’t attach to the bladder wall / lining or the urinary tract, they can’t cause bladder infection symptoms.”
Thanks for explaining a very
Thanks for explaining a very complex process as clearly as you have done. I’ve recently recovered from a, bad bladder bacteria infection. One of your articles recommended probiotics as a defense against such infections, but how does the good bacteria in a probiotic taken orally make it thru the filtration process of the kidneys and get to the bladder? Will not unwanted bacteria also get to the bladder by the same method?
Thanks, Edward
Oral probiotics are effective
Oral probiotics are effective for vaginal issues because the good bacteria end up colonizing in the digestive tract and migrating to the genital area with normal daily activity. This is not something most people think about, but it happens in women all the time because of the close proximity of the anus and vagina.
Very informative. Thanks for
Very informative. Thanks for your efforts.
Very helpful, thankyou
Very helpful, thankyou
HiJon, Thanks for a very
Hi Jon, Thanks for a very complete article on Urine. I recently saw a utube article on the health benefits of “drinking ones own urine, and fasting on distilled water.” Do you have any thoughts on the this? Regards
Jon covers this at the end of
Jon covers urine therapy at the end of this article: http://www.jonbarron.org/article/diseases-urinary-system
For information on fasting, check out Jon’s newsletter. http://www.jonbarron.org/detox/water-fasting-and-juice-fasting
Also, for more information on urine therapy, check out Coen van der Kroon’s book: “Golden Fountain: The Complete Guide to Urine Therapy Paperback.”
OMG…..thank you so much
OMG…..thank you so much this is a wonderful explanation. Its nicely written for one to quickly understand.
Cannot thank you to all who
Cannot thank you to all who put in the time and effort to write and revise this. A great read to understand the renal system and create a sturdy base to build knowledge on. So easy to follow yet so filled with important and detailed information. Thanks a million. Seriously…