
Every year it seems there’s another medical study testifying to the miraculous benefits of aspirin. It protects against heart disease and stroke, colon cancer, pancreatic cancer, and now, according to the latest studies, it may also help prevent skin, prostate, and lung cancers. The more one hears the more one begins to suspect that aspirin is the ultimate cure-all, the mythical “nectar of the gods.”
Then again, perhaps not. We’ve previously discussed how many of aspirin’s benefits are related to its ability to work as an anti-inflammatory — and there are better ways to get that effect. And other recent but less well publicized studies indicate more strongly than ever before (and as I have been saying for years) that aspirin doesn’t perform quite as well as advertised and that it comes with “aspirin side effects” that negate at least some of its questionable benefits.
Aspirin by itself is not really worth as many discussions as we’ve had on the subject; but the fact that the medical community, not to mention the aspirin manufacturers, keep finding ever new ways to promote the virtues of low-dose, daily aspirin means that we have to keep returning to the subject. With that in mind, let’s take a look at the most recent studies and see what they actually mean.
Aspirin and Skin Cancer
According to a study just published online in the journal CANCER, aspirin and the other commonly used NSAIDS (nonsteroidal anti-inflammatory drugs), which are most commonly used as pain killers, may also help protect against skin cancer.1 Johannesdottir, S. A., Chang, E. T., Mehnert, F., Schmidt, M., Olesen, A. B. and Sørensen, H. T. (2012), “Nonsteroidal anti-inflammatory drugs and the risk of skin cancer.” Cancer. Article first published online: 29 MAY 2012. <http://onlinelibrary.wiley.com/doi/10.1002/cncr.27406/abstract> This is in addition to the previous studies that have suggested that NSAIDs such as aspirin, ibuprofen, and naproxen can reduce the risk of developing colon cancer and pancreatic cancer.
 For example, earlier this year, two studies in The Lancet added to the evidence that a daily low dose of aspirin protects middle aged people against a number of cancers, particularly among those at higher risk. The first study established that aspirin reduced the risk of overall cancer death by 15% and that this reduction increased with prolonged use.2 Prof Peter M Rothwell, Jacqueline F Price, Prof F Gerald R Fowkes, et al. “Short-term effects of daily aspirin on cancer incidence, mortality, and non-vascular death: analysis of the time course of risks and benefits in 51 randomised controlled trials.” The Lancet, Volume 379, Issue 9826, Pages 1602 – 1612, 28 April 2012. For those who took it for five years or more, the reduced risk of death from cancer was 37%. The study also found that not only did aspirin reduce the risk of dying from cancer, it also reduced its incidence — 23% in men and 25% in women. The second study found that daily aspirin use also reduces the risk of metastasis, of the cancer spreading to distant organs, by about 40-50%.3 Prof Peter M Rothwell, Michelle Wilson, Jacqueline F Price, et al. “Effect of daily aspirin on risk of cancer metastasis: a study of incident cancers during randomised controlled trials.”The Lancet, Volume 379, Issue 9826, Pages 1591 – 1601, 28 April 2012. <http://www.thelancet.com/journals/lancet/article/PIIS0140-6736(12)60209-8/fulltext> This is particularly important because metastasis is what most commonly kills people who have cancer. The study also found that regular aspirin use reduced the risk of adenocarcinomas — common solid cancers such as colon, lung, and prostate cancer — by 46%. And in yet another recent study published in March in the British Journal of Cancer, researchers reported that colon cancer patients who take aspirin regularly shortly after diagnosis tend to live longer.4 E Bastiaannet, K Sampieri, O M Dekkers, A J M de Craen, G J Liefers, et al. “Use of Aspirin postdiagnosis improves survival for colon cancer patients.” British Journal of Cancer (2012) 106, 1564–1570. <http://www.nature.com/bjc/journal/v106/n9/pdf/bjc2012101a.pdf>
For example, earlier this year, two studies in The Lancet added to the evidence that a daily low dose of aspirin protects middle aged people against a number of cancers, particularly among those at higher risk. The first study established that aspirin reduced the risk of overall cancer death by 15% and that this reduction increased with prolonged use.2 Prof Peter M Rothwell, Jacqueline F Price, Prof F Gerald R Fowkes, et al. “Short-term effects of daily aspirin on cancer incidence, mortality, and non-vascular death: analysis of the time course of risks and benefits in 51 randomised controlled trials.” The Lancet, Volume 379, Issue 9826, Pages 1602 – 1612, 28 April 2012. For those who took it for five years or more, the reduced risk of death from cancer was 37%. The study also found that not only did aspirin reduce the risk of dying from cancer, it also reduced its incidence — 23% in men and 25% in women. The second study found that daily aspirin use also reduces the risk of metastasis, of the cancer spreading to distant organs, by about 40-50%.3 Prof Peter M Rothwell, Michelle Wilson, Jacqueline F Price, et al. “Effect of daily aspirin on risk of cancer metastasis: a study of incident cancers during randomised controlled trials.”The Lancet, Volume 379, Issue 9826, Pages 1591 – 1601, 28 April 2012. <http://www.thelancet.com/journals/lancet/article/PIIS0140-6736(12)60209-8/fulltext> This is particularly important because metastasis is what most commonly kills people who have cancer. The study also found that regular aspirin use reduced the risk of adenocarcinomas — common solid cancers such as colon, lung, and prostate cancer — by 46%. And in yet another recent study published in March in the British Journal of Cancer, researchers reported that colon cancer patients who take aspirin regularly shortly after diagnosis tend to live longer.4 E Bastiaannet, K Sampieri, O M Dekkers, A J M de Craen, G J Liefers, et al. “Use of Aspirin postdiagnosis improves survival for colon cancer patients.” British Journal of Cancer (2012) 106, 1564–1570. <http://www.nature.com/bjc/journal/v106/n9/pdf/bjc2012101a.pdf>
Which brings us to the Danish skin cancer study that prompted this newsletter. The results showed that:
- People with more than two prescriptions for NSAIDs had a 15% lower risk for squamous cell carcinoma and a 13% lower risk for malignant melanoma (two of the most common and deadliest skin cancers) than those with fewer than two prescriptions.
- The link was even stronger when the drugs were taken for seven years or more at a high intensity.
On the Other Hand, Aspirin Side Effects Include Bleeding
For people with a history of heart attacks or stroke, doctors generally are in agreement that taking aspirin is a key part of preventing a second “event.” The American Heart Association, the American Diabetes Association, and the U.S. Preventive Services Task Force all recommend daily, low-dose aspirin for people who are at a 20 percent increased risk of heart problems. According to medical groupthink, the benefits of preventing a second heart attack outweigh the risks of bleeding for most people. But there is a fly in the ointment. Despite the medical bandwagon for aspirin, doctors have known for years that aspirin, in fact all NSAIDS, increase the risk of intestinal and cranial bleeding. “No preventive approach is without risk,” said Dr. Thomas Schwenk, Dean of the University Of Nevada School Of Medicine. “If the benefits are barely measurable but the risks are real and possibly greater, then the decision making may shift against the use of aspirin.”
I know that sometimes we tend to think of the medical community as a giant monolith functioning in total lockstep. But that’s not exactly true. Dissenting voices do appear. Unfortunately, medical groupthink is like a giant oil tanker; it can take many miles to get it to change course. For example, it took almost 100 years and numerous medical studies proving that it was no more effective than a simple lumpectomy before radical mastectomies were finally dethroned as the dominant medical procedure for breast cancer — to the point where they are now rarely used. In some ways, watching the medical community deal with challenges to accepted belief is like watching a patient go through the five stages of grief — denial, anger, bargaining, depression, and acceptance. As you will see, when it comes to aspirin, as with statin drugs, we have already gone through denial and anger; we are now in the bargaining stage.
In fact, when it comes to the low-dose, daily aspirin, there are many dissenters. And while it is true that millions of people still take aspirin every day to lower their heart attack and stroke risk (thank you very much television advertising), not to mention a whole new crop who may yet be harvested and convinced to do so to “prevent cancer,” persistent research is starting to change some of that thinking. And a major study just published in the Journal of the American Medical Association has only added to the fire. According to the results involving 186,425 people using low-dose aspirin and a matching control group of 186,425 that did not, aspirin use was “significantly” associated with an increased risk of major gastrointestinal and cerebral bleeding episodes.5 De Berardis G, Lucisano G, D’Ettorre A, et al. “Association of aspirin use with major bleeding in patients with and without diabetes.” JAMA. 2012;307(21):2286-2294. <http://jama.jamanetwork.com/article.aspx?articleID=1172042> The risk for serious bleeds was a stunning five times higher than had previously been reported in clinical trials of daily, low-dose aspirin regimens.
Curiously, the researchers also found that patients with diabetes had a 36% increased risk for these same potentially life-threatening bleeding episodes — even when they did not take aspirin. Aspirin use did not appear to influence this risk for people with diabetes one way or another. The finding that diabetes in and of itself conveys a risk for bleeding is new — and needs to be explored in a future newsletter.
Bargaining
If this study is correct, the use of daily, low-dose aspirin increases your risk of internal bleeding by as much as 500%. This has to present a conflict for all those doctors who prescribe (and patients who use) daily aspirin for heart health — at least if they have no definitive risk factors. The obvious rationalization to accept aspirin side effects is that the risk of dying from a heart attack is much greater than the risk of dying from internal bleeding.
The evidence in favor of their argument seems incontrovertible. According to previous studies, low-dose aspirin lowers your risk of having a heart attack by 60 percent.6 Ryan Jaslow, “Taking daily aspirin to prevent a heart attack? Don’t stop, warn doctors.” CBS News Health Pop. July 21, 2011 (Accessed 11 June 12.) <http://www.cbsnews.com/8301-504763_162-20081379-10391704.html> That’s impressive! Unfortunately, statistics are not always what they seem. As it turns out, aspirin’s proclivities when it comes to heart disease are very similar to those seen with statin drugs. Yes, they reduce your risk of having a “second” heart attack or stroke, but what does that mean? First of all, when it comes to the treatment’s usefulness for preventing a first heart attack or stroke, the benefits seem to vanish. And more importantly, as also seen with statin drugs, although aspirin reduces your risk of having a “second” event, it does not necessarily decrease your risk of dying — not even one single percent. And isn’t that really what you’re trying to prevent? In fact, a number of studies have shown that there is no significant association between using or not using low-dose aspirin and the risk of death from coronary heart disease.7 Luis A García Rodríguez, Lucía Cea-Soriano, Elisa Martín-Merino, Saga Johansson. “Discontinuation of low dose aspirin and risk of myocardial infarction: case-control study in UK primary care.” BMJ 2011;343:d4094. <http://www.bmj.com/content/343/bmj.d4094> Ouch!
So how does the medical community handle these contradictions?
According to Dr. Antonio Nicolucci, one of the “bleeding study” authors, “People with a moderate-to-high risk for having a major cardiovascular event probably benefit from aspirin therapy, but the risks may outweigh the benefits for people with a lower risk.”
In an editorial accompanying publication of the study, Dr. Jolanta Siller-Matula, of the Medical University of Vienna, laid out the numbers. For a hypothetical group of 10,000 patients, aspirin used to prevent a second heart attack or stroke would prevent about 250 major vascular events and would cause about 40 cases of brain bleeding. “Thus the net benefit of aspirin for secondary prevention would substantially exceed the bleeding hazard,” she wrote. However, for those at a lower risk of heart disease, such as people who have some risk factors but have never had a heart attack, she said that for 10,000 of those patients, aspirin would be expected to prevent seven major vascular events, but cause hemorrhagic stroke and extra-cranial bleeding in another four patients.8 Jolanta M. Siller-Matula, “Hemorrhagic Complications Associated With AspirinAn Underestimated Hazard in Clinical Practice?” JAMA. 2012;307(21):2318-2320. doi:10.1001/jama.2012.6152 <http://jama.jamanetwork.com/article.aspx?articleid=1172021>
As might be expected, the pro aspirin camp couldn’t let things lie there. They point out that the study also suggests a protective role for cholesterol-lowering statin drugs against bleeding. Specifically, the study noted that the use of statins was associated with a “significant reduction” in both GI and intracranial bleeding. On the other hand, they also noted that this might be due to the concomitant use of proton pump inhibitors such as Prilosec (to prevent heartburn), quite common in this population. In any case, some in the medical community have leaped to the conclusion that it might be best to now recommend the simultaneous use of statin drugs and low-dose aspirin together — to double the bang for your buck as it were. But of course, they already do.9 Michael Hoffmeister, Jenny Chang-Claude, and Hermann Brenner. “Individual and joint use of statins and low-dose aspirin and risk of colorectal cancer: A population-based case–control study.” Int. J. Cancer: 121, 1325–1330 (2007) <http://onlinelibrary.wiley.com/doi/10.1002/ijc.22796/pdf> In fact, it is more common than not.
Natural Alternatives to Aspirin
We now know what the medical community says about aspirin and the other NSAIDS and how the most recent studies have charged the dialogue on both sides of the medical debate. But is there something we can extrapolate from all of these studies that might point us in an entirely different direction — a more natural alternative to aspirin, perhaps?
And the answer is “yes.”
Lessons from the Skin Cancer Study
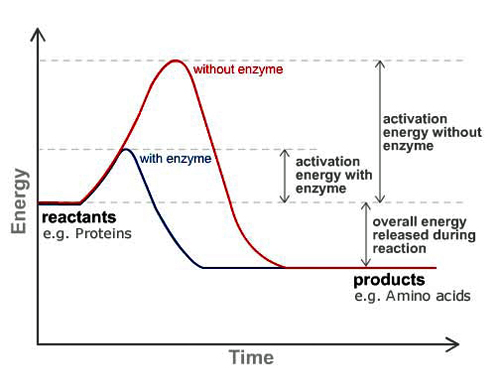
It is important to remember that the skin cancer study found equal benefits for all the commonly used NSAID painkillers, not just aspirin. So what do aspirin, ibuprofen, and naproxen all have in common? They are all anti-inflammatories. They systemically reduce inflammation throughout the body. Their generic name — nonsteroidal anti-inflammatory drugs — describes what they do.
 Virtually all of the benefits associated with aspirin and the other NSAIDS stem from their ability to inhibit your body’s production of prostaglandins. Prostaglandins are like hormones in that they work to direct responses in the human body. For example, prostaglandins play a role in directing the body’s pain and inflammation response to injury. They help control how fast blood clots in response to a wound, or how readily plaque is formed when there is damage to an arterial wall. They also play a role in directing uterine contractions, not to mention your body’s immune response, and even aspects of metabolism. Aspirin and NSAIDS such as ibuprofen and Motrin work by decreasing prostaglandin levels. They do this by inhibiting the production of the cyclooxygenase enzyme COX-2. Specifically, if you inhibit COX-2, you inhibit the production of prostaglandins. In summary, NSAIDS are COX-2 inhibitors, which results in reduced inflammation.
Virtually all of the benefits associated with aspirin and the other NSAIDS stem from their ability to inhibit your body’s production of prostaglandins. Prostaglandins are like hormones in that they work to direct responses in the human body. For example, prostaglandins play a role in directing the body’s pain and inflammation response to injury. They help control how fast blood clots in response to a wound, or how readily plaque is formed when there is damage to an arterial wall. They also play a role in directing uterine contractions, not to mention your body’s immune response, and even aspects of metabolism. Aspirin and NSAIDS such as ibuprofen and Motrin work by decreasing prostaglandin levels. They do this by inhibiting the production of the cyclooxygenase enzyme COX-2. Specifically, if you inhibit COX-2, you inhibit the production of prostaglandins. In summary, NSAIDS are COX-2 inhibitors, which results in reduced inflammation.
Reducing inflammation diminishes your chances of getting all different types of cancer in two ways — at least according to my theories on the disease.
First, inflammation reduces circulation — of blood, lymph, and energy. Reduced circulation of blood negatively impacts cells in a number of ways. It:
- Weakens cells by denying them the nutrients they need, which can lead to cellular mutation
- Allows toxins to build up in cells, which can lead to cellular mutation
- Denies cells access to adequate supplies of oxygen, which can lead to cellular mutation
- It raises cellular pH by allowing CO2 levels to rise inside cells, which can increase cellular mutation
Second, the reduced circulation of lymph allows toxins to build up in the body, which can negatively impact the health of cells, thus leading to increased cellular mutation. Your lymph is your body’s sewer system, and like any sewer system, what doesn’t circulate accumulates. And accumulated sewage is toxic to all who come in contact with it. Incidentally, whereas the cardiovascular system has a pump (the heart) to move fluid (blood) through the system, the lymphatic system does not. It relies on the contraction of muscles to move lymph throughout the body, although the larger lymph vessels have a layer of smooth muscle in their walls that contracts rhythmically to help “pump” lymph along. But it is primarily the contraction of skeletal muscles, brought about by simple body movement and the mechanics of breathing that move lymph on its way. Thus, any inflammation in muscle tissue reduces the movement of lymph through that tissue.
Third, the reduced ability of energy to circulate in the body can cause cellular energy levels to drop, which has been medically associated with an increased tendency for cells to turn cancerous.
On a different note, inflammation in and of itself is a stress factor that can lead to epigenetic changes in cellular DNA.
The bottom line is that anything that reduces systemic inflammation is likely to reduce your incidence of many types of cancer for all of the reasons cited above. All of the NSAIDS, including aspirin, do that; thus, it is not surprising that all of the NSAIDS show statistical benefit in reducing the incidence cancer.
Aspirin and Heart Disease
When it comes to heart disease, aspirin is unique among the NSAIDs in that it is the only NSAID that inhibits the clotting of blood for a prolonged period (4 to 7 days). Most NSAIDs inhibit the clotting of blood for only a few hours. How does aspirin do this?
Aspirin inhibits both COX-1 and COX-2. We’ve already discussed the function of COX-2 and the role it plays in driving pain and inflammation in response to cell damage and tissue injury. COX-1, on the other hand, has nothing to do with pain; instead, it is primarily a “housekeeping” enzyme, helping to regulate everyday functions in the body — one of which is blood clotting. If you inhibit the production of COX-1, which aspirin does, you reduce the production of platelet aggregating factor thromboxane A2, which means you have less chance of forming blood clots in the arteries — thus a reduced chance of having heart attacks and strokes.
But this brings up the question that we have already danced around.
Studies have shown that long-term daily use of low-dose aspirin may indeed lower the risk of “second” heart attacks and strokes caused by blockages, but it does not appear to reduce the risk of dying from these problems. The question, then, is what might account for this paradox? First heart attacks are usually the result of hardening and narrowing of the arteries — something aspirin has no impact on. Second heart attacks, however, are often the result of blood clots forming at points of cardiovascular injury and lodging in already narrowed arteries — something aspirin can help with by virtue of its ability to thin the blood.
Note: COX-1 has one other important function. It is responsible for the proper functioning of the stomach and intestinal lining. Specifically, it promotes the production of the natural mucus lining that protects the stomach, the duodenum, and the small intestine. If you inhibit COX-1, as aspirin does, you compromise the integrity of the intestinal tract. The result, of course, is micro-bleeding in the gastrointestinal tract. In effect, aspirin’s ability to inhibit COX-1 is a mixed blessing — helpful in one way and harmful in two.
Conclusion
Putting this altogether, we arrive at the real question of the moment: is there a safe, all-natural alternative to aspirin and the other NSAIDS for protecting us from cancer and heart disease, without the negative side effects? We’re looking for something all natural that:
- Reduces systemic inflammation at least as well as the NSAIDS
- Reduces the tendency of blood to inappropriately clot in unhealthy places such as the coronary arteries and the brain — thus reducing the likelihood of cardiovascular events
- Does not damage the intestinal lining, thus having no issues with gastrointestinal bleeding
- Does not damage the brain’s vascular system, thereby not contributing to hemorrhagic stroke
- And for good measure can help dissolve arterial plaque and scarring
- Improve lung function in people with COPD
- And, for good measure, dissolve dental plaque
In other words, we’re talking about systemic proteolytic enzymes — enzymes designed to be taken between meals so that they quickly enter the bloodstream (as opposed to being involved in the digestion of food) where they can indeed reduce systemic inflammation, lessen pain, optimize the ability of blood cells to move independently, lower the risk of cell mutations, and help repair cardiovascular damage.
And on top of everything else, proteolytic enzymes can help prevent against deep vein thrombosis resulting from long periods of sitting — something aspirin cannot do.
The difference between proteolytic enzymes and NSAIDS
The obvious issue that one has to be concerned with at this point is that if proteolytic enzymes and NSAIDS do so many of the same things — reducing pain, inflammation, risk of coronary events, and risk of cancer — how are they different? Are proteolytic enzymes just natural versions of NSAIDS, complete with many of the same problems? And the answer is: not at all. They work on the same things but in entirely different ways. And it is that difference that makes proteolytic enzymes the better choice.
As we’ve already discussed, aspirin and the other NSAIDS work by decreasing prostaglandin levels. They do this by inhibiting the production of the cyclooxygenase enzymes — both COX-1 and COX-2. But all of these bio chemicals — prostaglandin and the cyclooxygenase enzymes — have important functions in the body. If you “shut down” their production, you shut down crucial systems as well as excess inflammation. As you may remember from earlier, COX-1 is responsible for the proper functioning of the stomach and intestinal lining. If you inhibit its production, you compromise the integrity of the intestinal tract. The result, of course, is micro-bleeding in the gut.
Proteolytic enzymes, on the other hand, work further down the chain of events. They are not COX inhibitors. Instead, they catalyze the breakdown of excess and inappropriate proteins floating around in your bloodstream. This includes bacteria, allergens, and prostaglandins. Proteolytic enzymes don’t disrupt the normal cycle; they merely clean up the excesses produced by that system. By cleaning up excess prostaglandins, they reduce pain and inflammation. By breaking down fibrin, the clotting protein, they prevent the formation of dangerous clots in the bloodstream — even clots formed as the result of DVT, something aspirin can’t do. To put this in more prosaic terms: aspirin is a sledgehammer — proteolytic enzymes, a surgeoun’s scalpel. (By the way, you need to stop taking proteolytic enzymes several days before surgery as they will tend to increase bleeding — not excessively, but noticeably.)
It should also be mentioned that it is the ability of proteolytic enzymes to break down proteins that helps them break up mucous in the lungs and plaque on your teeth — not to mention helping break down arterial scar tissue and plaque. (Mucous is made from a combination of sugars and proteins. The protective coating on dental plaque is comprised of proteins, sugars, and fats. And scar tissue is almost entirely protein, whereas arterial plaque is comprised of cholesterol, minerals, and blood platelets — all bound together by proteins.)
Are proteolytic enzymes perfectly safe? Nothing is perfectly safe. Heck, if you overdose on water, it can kill you — a condition called hyponatremia. (Don’t panic; it’s difficult to do.) So what is the danger associated with proteolytic enzymes? Theoretically, they can increase your risk of suffering a hemorrhagic stroke. There are two main types of stroke — ischemic and hemorrhagic. Ischemic stroke is far more common and occurs when blood flow to a part or parts of the brain is stopped by a blockage in a vessel. This is the type of stroke that most people think of when they use the word “stoke.” One of the primary reasons for using blood thinners is to prevent this type of stroke. Like aspirin, proteolytic enzymes actually help prevent this type of stroke. Hemorrhagic stroke, on the other hand, is more deadly and occurs when a weakened vessel tears or ruptures, diverting blood flow from its normal course and, instead, leaking or spilling it into or around the brain itself. Proteolytic enzymes don’t cause this type of stroke, but the thinner your blood is when you have one, the faster the blood may leak out into the brain and the more damaging the results. Unless you have a known risk for this type of stroke, it is not a reason to avoid keeping your blood optimized. You are far more likely to succumb to overly thick, clotted blood.
 But even in this regard, proteolytic enzymes are far safer and more protective than aspirin. Aspirin not only thins the blood as do proteolytic enzymes, but aspirin actually contributes its own risk factor above and beyond thinner blood. One of the causes of brain bleeding is excessive protein deposits in the blood vessel walls. Multiple studies have determined that the most prominent cause of protein deposits in the brain have been linked to drugs like aspirin.10 Philip B. Gorelick. “Cerebral Microbleeds Evidence of Heightened Risk Associated With Aspirin Use.” Arch Neurol. 2009;66(6):691-693 <http://archneur.jamanetwork.com/pdfaccess.ashx?ResourceID=1403204&PDFSource=13> Researchers that studied brain scans of more than a thousand people found that 70% of those that took aspirin had microscopic bleeding in the brain.11 Vernooij MW, Haag MDM, van der Lugt A. et al. “Use of antithrombotic drugs and the presence of cerebral microbleeds: the Rotterdam Scan Study.” Arch Neurol 2009;66 (6) 714- 720. <http://archneur.jamanetwork.com/pdfaccess.ashx?ResourceID=1403437&PDFSource=13>
But even in this regard, proteolytic enzymes are far safer and more protective than aspirin. Aspirin not only thins the blood as do proteolytic enzymes, but aspirin actually contributes its own risk factor above and beyond thinner blood. One of the causes of brain bleeding is excessive protein deposits in the blood vessel walls. Multiple studies have determined that the most prominent cause of protein deposits in the brain have been linked to drugs like aspirin.10 Philip B. Gorelick. “Cerebral Microbleeds Evidence of Heightened Risk Associated With Aspirin Use.” Arch Neurol. 2009;66(6):691-693 <http://archneur.jamanetwork.com/pdfaccess.ashx?ResourceID=1403204&PDFSource=13> Researchers that studied brain scans of more than a thousand people found that 70% of those that took aspirin had microscopic bleeding in the brain.11 Vernooij MW, Haag MDM, van der Lugt A. et al. “Use of antithrombotic drugs and the presence of cerebral microbleeds: the Rotterdam Scan Study.” Arch Neurol 2009;66 (6) 714- 720. <http://archneur.jamanetwork.com/pdfaccess.ashx?ResourceID=1403437&PDFSource=13>
Systemic proteolytic enzymes not only don’t cause excessive protein deposits to form in the brain’s blood vessel walls, they actually work to break down any such deposits! All in all, proteolytic enzymes are a safer, more effective alternative for everything that NSAIDS do than NSAIDS themselves. For more information on systemic proteolytic enzymes, check out: /enzymes/natural-health-remedies-proteolytic-systemic
References
| ↑1 | Johannesdottir, S. A., Chang, E. T., Mehnert, F., Schmidt, M., Olesen, A. B. and Sørensen, H. T. (2012), “Nonsteroidal anti-inflammatory drugs and the risk of skin cancer.” Cancer. Article first published online: 29 MAY 2012. <http://onlinelibrary.wiley.com/doi/10.1002/cncr.27406/abstract> |
|---|---|
| ↑2 | Prof Peter M Rothwell, Jacqueline F Price, Prof F Gerald R Fowkes, et al. “Short-term effects of daily aspirin on cancer incidence, mortality, and non-vascular death: analysis of the time course of risks and benefits in 51 randomised controlled trials.” The Lancet, Volume 379, Issue 9826, Pages 1602 – 1612, 28 April 2012. |
| ↑3 | Prof Peter M Rothwell, Michelle Wilson, Jacqueline F Price, et al. “Effect of daily aspirin on risk of cancer metastasis: a study of incident cancers during randomised controlled trials.”The Lancet, Volume 379, Issue 9826, Pages 1591 – 1601, 28 April 2012. <http://www.thelancet.com/journals/lancet/article/PIIS0140-6736(12)60209-8/fulltext> |
| ↑4 | E Bastiaannet, K Sampieri, O M Dekkers, A J M de Craen, G J Liefers, et al. “Use of Aspirin postdiagnosis improves survival for colon cancer patients.” British Journal of Cancer (2012) 106, 1564–1570. <http://www.nature.com/bjc/journal/v106/n9/pdf/bjc2012101a.pdf> |
| ↑5 | De Berardis G, Lucisano G, D’Ettorre A, et al. “Association of aspirin use with major bleeding in patients with and without diabetes.” JAMA. 2012;307(21):2286-2294. <http://jama.jamanetwork.com/article.aspx?articleID=1172042> |
| ↑6 | Ryan Jaslow, “Taking daily aspirin to prevent a heart attack? Don’t stop, warn doctors.” CBS News Health Pop. July 21, 2011 (Accessed 11 June 12.) <http://www.cbsnews.com/8301-504763_162-20081379-10391704.html> |
| ↑7 | Luis A García Rodríguez, Lucía Cea-Soriano, Elisa Martín-Merino, Saga Johansson. “Discontinuation of low dose aspirin and risk of myocardial infarction: case-control study in UK primary care.” BMJ 2011;343:d4094. <http://www.bmj.com/content/343/bmj.d4094> |
| ↑8 | Jolanta M. Siller-Matula, “Hemorrhagic Complications Associated With AspirinAn Underestimated Hazard in Clinical Practice?” JAMA. 2012;307(21):2318-2320. doi:10.1001/jama.2012.6152 <http://jama.jamanetwork.com/article.aspx?articleid=1172021> |
| ↑9 | Michael Hoffmeister, Jenny Chang-Claude, and Hermann Brenner. “Individual and joint use of statins and low-dose aspirin and risk of colorectal cancer: A population-based case–control study.” Int. J. Cancer: 121, 1325–1330 (2007) <http://onlinelibrary.wiley.com/doi/10.1002/ijc.22796/pdf> |
| ↑10 | Philip B. Gorelick. “Cerebral Microbleeds Evidence of Heightened Risk Associated With Aspirin Use.” Arch Neurol. 2009;66(6):691-693 <http://archneur.jamanetwork.com/pdfaccess.ashx?ResourceID=1403204&PDFSource=13> |
| ↑11 | Vernooij MW, Haag MDM, van der Lugt A. et al. “Use of antithrombotic drugs and the presence of cerebral microbleeds: the Rotterdam Scan Study.” Arch Neurol 2009;66 (6) 714- 720. <http://archneur.jamanetwork.com/pdfaccess.ashx?ResourceID=1403437&PDFSource=13> |






Do you have any comments on
Do you have any comments on the coated low dos asprin. Is this a better option for stomach protection?
It might protect your stomach
It might protect your stomach a bit, but it won't do anything to protect the rest of your intestinal tract. (You might want to read the next comment, which talks about aspirin and duodenal ulcers.) But keep in mind, the real problem isn't caused by aspirin "touching" your stomach or intestinal tissue. It's caused by aspirin working as a Cox-1 inhibitor, which suppresses mucous formation thourhgout your intestinal tract. That happens when apsirin gets into your bloodstream where it ultimately circulates back to your stomach and intestinal tissue, so coating aspirin makes no difference in that regard.
One of the most disturbing
One of the most disturbing experiences in my nursing career was answering a call light of an 8-y/o little girl who was admitted for treatment of her rheumatoid arthritis and was on aspirin therapy. When I entered her room, she was extremely pale and complained of a headache, holding a hand against her temple, then began to retch. I grabbed the nearest receptical, a stainless steel wash basin, which this unfortunate child proceeded to fill halfway up with fresh blood and clots. She very nearly died that night due to the severe erosion to her GI tract.
The next day I had my 9 y/o son in the doctor’s office (same doctor). I advised him that I’d had his little patient the night before and then told him cryptically that my son didn’t like pizza or bacon anymore. He just looked a long time at me then inquired of my son, “Why not; all guys like that stuff…” My son replied, “It hurts my stomach…” (He had taken aspirin, too, though certainly not at the same level as my little patient.). Tests revealed that my 9 y/o already had a deep duodenal ulcer the size of a dime; thankfully it had not perforated. So, we stopped using aspirin at our house and the last time I used it was just before I developed several deep bruises for no explainable reason, including one that became a true hematoma.
I would have to have very strong motivation to use aspirin ever again. Frankly, I can’t think of a good enough reason to do so.
I also read a report which
I also read a report which stated that aspirin thins the blood by killing off the red blood cells. There’s a much easier way to thin the blood… drink water!!
Hi Jon
What about the extract
Hi Jon
What about the extract from white willow bark, is this a safer alternative to aspirin? Is there any other plant substance in nature like willow bark that effectively functions like/better than aspirin, without its side-effects? Thanks.
Actually, Jon talks about the
Actually, Jon talks about the differences between white willow bark and aspirin in some detail in the very first link in the article above (http://www.jonbarron.org/natural-health/aspirin-cancer-dangers-risks). To summarize from that discussion, “Salicin, the natural healing compound found in white willow bark and synthesized acetylsalicylic acid are not the same thing — not remotely. Salicin does a far better job shielding the body from the acid effects of the molecule.” However, that said, white willow bark still works as both a Cox-2 AND a Cox-1 inhibitor, so you still have that problem. Proteolytic enzymes would still be the preferred choice.
OK, thanks very much for
OK, thanks very much for that. I think I’ve got information overload, I have got that aspirin article from Jon you mentioned (I’m subscribed to Jon’s health e-mails), it’s buried in the 3000 or so other health files I’ve got on my computer.
I do find that a quarter aspirin helps me sleep somewhat better (whereas 10 mg of melatonin does absolutely nothing for me – maybe I should have tried 20 mg), and 500 mg of GABA is also totally useless.
It’s a pity Jon doesn’t have a rep in England so that we can buy his stuff locally (rather than getting it direct from the USA).
If the proteolytic enzymes
If the proteolytic enzymes are so much better than aspirin, why then are they not sold on the market? I have never heard of them before.
You must be new to
You must be new to alternative health. Proteolytic enzymes such as nattokinase, serrapeptase, Seaprose-S, and lumbrokinase are well studied, easily available in the market, and have been used for years for their ability to prevent blood clots and reduce inflammation. Search any of them on the net and see for yourself. As a side note, Jon prefers well designed proteolytic enzyme formulas (http://www.jonbarron.org/enzymes/natural-health-remedies-proteolytic-systemic), as opposed to single ingredient enzyme supplements.
Thank you so much for whyever
Thank you so much for whyever you wrote this article just now. I’ve been searching for alternatives for my 14 yo granddaughter with cystic fibrosis and the arthritis that can come with it. I’m assuming that your P. enzymes would help with both the mucus and the pain. She is on a heavy enzyme dosage, but with meals, and, much to our grief, Naprosyn x times a day. Can you take them simultaneously until ..?? How would I figure out dosage for her? We’re all familiar with white willow bark, but yours has been the best explantion of it’s pros & cons. Much, Much thanx!
For obvious legal reasons, we
For obvious legal reasons, we cannot diagnose or prescribe for specific medical conditions – merely provide information. With that in mind, you would need to talk to your granddaughter’s physician. If they were willing to give it a try, the usual rule on starting levels for a child is to calculate a full serving as being appropriate for a person of 150 lbs. Then pro rate accordingly. For example, you would start at half the recommended serving for a child of 75 lbs. Then adjust up or down as desired.
Is there any evidence
Is there any evidence supporting the efficacy of proteolytic enzymes against autoimmune diseases? My wife has polymyalgia rheumatica (PMR). From all the researching I have done, it would seem that any powerful anti-inflammatory might — *might* — have some chance of offering a curative or palliative effect. So far the standard ones have offered any detectable relief.
Is there a danger that the
Is there a danger that the enzymes may disolve a loosely attached plaque in the arteries and thus cause a blockage.
You might want to search the
You might want to search the site for what Jon has to say about immunomodulators. For example: http://www.jonbarron.org/immunity/anatomy-physiology-optimizing-immune-system
Thank you for the reference.
Thank you for the reference. It does suggest alternative approaches to the disease, besides anti-inflammatory agents per se.
There is probably a greater
There is probably a greater danger that a “loosely attached plaque” will break free intact and cause a blockage, rather than a “dissolved” plaque causing a problem, wouldn’t you think?
Has Jon done any health
Has Jon done any health series on eye health (I couldn’t find any), including on conditions like Posterior Vitreous Detachment and what natural products to take for it, as well as anti-ageing eye health products?
This is a very interesting
This is a very interesting article, but one huge factor is not discussed….cost. I have researched good proteolytic enzyme formulas several times in the past and each time I have been totally shocked at the price of these supplements. I don’t take aspirin myself, but the cost of taking a daily aspirin is miniscule compared to the cost of taking these enzymes on a daily basis. If money is no object, then fine, go for the proteolytic enzymes. If you live in the real world, you’re going to throw up your hands in disgust at their cost and just take an aspirin !
Really? You would choose
Really? You would choose gastrointestinal and cerebral bleeding over 30-60 cents a day for proteolytic enzymes? In the real world, where people spend $3.00 for a cup of coffee without batting an eye, I think many people would consider proteolytic enzymes a real bargain.
Stay tuned and watch for the
Stay tuned and watch for the newsletter, that is still coming!