The first official death from COVID-19 was announced by President Trump on the last day of February 2020. Although we now know that people in the United States were actually dying weeks if not several months earlier, official record keeping of COVID deaths did not begin until the last day of February. What this means is that this coming March will mark the end of the first year of recorded deaths for COVID in the U.S. This is important since, if you want to compare the impact of COVID to other causes of death in the U.S., you need to calculate its impact over 12 months as all other causes of death are calculated. An apples-to-apples thing. For COVID, then, we’re essentially talking about using the numbers from March 1, 2020, to February 28, 2021.
That said, and despite the December roll out of the first COVID vaccines, February is going to be a horrible month when it comes to COVID, with the one-year total for deaths blasting past 500,000, and the one-year total of people suffering from the long-term effects of COVID possibly hitting as high as 18 million if the latest research is correct (more on this later). This slots COVID solidly into the third spot for causes of death in the U.S., with accidents trailing far behind in the fourth position at 167,000 deaths. 1 “Leading Causes of Death.” CDC National Center for Disease Control. October 30, 2020. (Accessed 18 Jan 2021.)
- Heart disease: 655,381
- Cancer: 599,274
- Accidents (unintentional injuries): 167,127
- Chronic lower respiratory diseases: 159,486
- Stroke (cerebrovascular diseases): 147,810
- Alzheimer’s disease: 122,019
- Diabetes: 84,946
- Influenza and pneumonia: 59,120
- Nephritis, nephrotic syndrome, and nephrosis: 51,386
- Intentional self-harm (suicide): 48,344
Now, before we go on, let me address an important issue here. Every time I write about COVID, a number of people write in to tell me that as much as they enjoy my newsletters, when it comes to COVID, I have been duped by the deep state, that COVID is nowhere near as deadly as claimed and that the number of reported deaths is greatly exaggerated. They know this because they work in the healthcare industry or they know someone who works in the industry who told them that it’s true or they have “seen the video.”
So, what’s my point?
 My first newsletter on COVID was published on February 27th, two days before President Trump announced the first death. Back then, the President, the CDC, and the entire apparatus of the “deep state” were publicly saying that COVID would be contained, that few people would die, lockdowns were unnecessary, and wearing masks would not help. In my newsletter, on the contrary, I predicted:
My first newsletter on COVID was published on February 27th, two days before President Trump announced the first death. Back then, the President, the CDC, and the entire apparatus of the “deep state” were publicly saying that COVID would be contained, that few people would die, lockdowns were unnecessary, and wearing masks would not help. In my newsletter, on the contrary, I predicted:
“Small percentages of people being critically ill and dying works out to be very large numbers if applied across enough people.”
Which is exactly what we’ve seen.
“Because the current coronavirus can be asymptomatic, or at least very mild, there’s a better chance people will be going about their day as normal unknowingly spreading infection. Additionally, because people won’t know when they started spreading infection, it will be that much harder to trace and prevent the disease from spreading to others.”
Which again is exactly what we’ve seen.
“There’s an emerging consensus that the outbreak will eventually morph into a new seasonal disease, which, per The Atlantic, could one day turn ‘cold and flu season’ into ‘cold and flu and COVID-19 season.’”
Which we will talk about in a bit.
The point is that I was predicting these outcomes before the “deep state” was predicting them, so you cannot really claim I was duped by the deep state. In other words, claiming that I was duped by the deep state is a non-starter.
But let’s pretend for a moment that the number of deaths is, as claimed by many, greatly exaggerated. (They are not, of course. I explained back in my August newsletter how the cause of death is determined and how someone can die from a heart attack but legitimately have the cause of death listed as COVID because COVID triggered the heart attack. This is how the cause of death has been determined for decades.) But anyway, let’s pretend for a moment that the number of COVID deaths is greatly exaggerated—say 10%, 20%, 30%, 40%, even 100% exaggerated. Let’s say the deep state is literally doubling the number of actual deaths from COVID in their statistics. That means you would still have over 250,000 deaths from COVID in the 12 months from March1, 2020 to February 28, 2021. Even then, even if the deep state lied and doubled the number of actual deaths, COVID would still be solidly ensconced as the third leading cause of death in the United States over the last year. In other words, even if it is a hoax (which it’s not), it’s a very, very, very deadly hoax.
But There’s Another Way to Look at These Numbers
COVID aside, 2020 was the deadliest year in U.S. history, with preliminary numbers suggesting that the United States saw more than 3.2 million deaths for the year, or at least 400,000 more than in 2019. Incidentally, this would mark the first time in U.S. history that deaths topped 3 million. Now, while it is true that U.S. deaths do increase slightly most years simply as a result of an ever-growing population, the 2020 increase would mark the largest single-year percentage leap since 1918, the year, coincidentally, of the last great pandemic. According to the numbers out of Johns Hopkins, 318,000 of those 400,000 (again, this is through December 31st) have been tagged as the result of COVID. The other 82,000 are unaccounted for. They might be COVID but have not been definitively identified as such. What we do know is that they are not the result of increased heart attacks or cancer, as those numbers have actually held steady or decreased for the last several years.
Now, here’s the point. If COVID is a hoax as has been proposed by many, the alternative is far, far worse—far more terrifying. We would now be talking about 318-400 thousand deaths in 2020 that would have no known cause. It might be a virus other than COVID, an unidentified bacterium, chemtrails, alien death rays. But that’s all speculation. If it is not COVID, then the cause is unknown. And if the cause is unknown, then there is nothing we can do about it other than get sick and die. So, if that’s the alternative, I certainly hope it’s not a hoax and that it really is the result of the COVID pandemic, and that the medical community is on the right track in trying to defend against it. Otherwise, as Geena Davis said in The Fly, “Be afraid. Be very afraid.” If COVID is really a hoax, that means we would have no idea what’s killing us and no idea how to prevent it from doing so. We would have to list the third leading cause of death in the U.S. as “bad luck.”
I understand that nothing I have said will change the minds of anyone who “has seen the video” or has a close friend who has seen the video, whichever one of a number of them circulating on the net claiming that COVID is a hoax. In fact, I should probably take a hint from ex-GOP pollster Frank Luntz, who recently announced, after a focus group he was conducting went off the rails when discussing COVID, “I reached a point where I don’t want to do this anymore.” 2 Jake Lahut “Ex-GOP pollster Frank Luntz says ‘I don’t want to do this anymore’ after ‘unity’ themed focus group goes off the rails.” Business Insider. 21 Jan 2021. (Accessed 21 Jan 2021.)
But, as it turns out, I guess I’m a glutton for punishment. So, for those of you still open to the possibility that the threat from COVID is real, let’s continue.
Doesn’t Having a Strong Immune System Protect You from COVID?
If only it were that simple!
Having a strong immune system is important and can indeed be helpful when dealing with COVID 19, but it is no guarantee that you will not get COVID, become a COVID long-hauler, or die.
When people are talking about a strong immune system, they are usually talking about a strong innate immune system, the part of your immune system that is boosted by proper diet, exercise, and supplementation. Your innate immune system includes the nonspecific defense mechanisms that come into play immediately or within hours of a pathogen’s appearance in the body. But because it is nonspecific, it can only offer a limited defense against many pathogens.
As I explained last April, when it comes to COVID, what you really need is a trained adaptive immune system. Adaptive immunity refers to pathogen specific immune responses. The adaptive immune response is more complex and magnitudes more robust than the innate. This is where antibodies come into play, for example. But for the adaptive immune system to act, the antigen/pathogen that it is defending against must first be processed and recognized. Once an antigen has been recognized, the adaptive immune system creates an army of antibodies and immune cells specifically designed to attack that antigen. Adaptive immunity also includes a “memory” that makes future responses against a specific antigen more efficient. The thing is, you cannot build a strong adaptive immune system through diet and exercise alone, it requires exposure to the infecting pathogen either by contracting COVID itself or by being exposed to key proteins from the virus through vaccination. Without one of those two conditions having been met, the most powerful part of your immune system will sit idly by when you contract COVID—at least for the first two weeks of infection, and by then, it is often too late.
Also, when it comes to COVID, there are several complicating factors that can undermine the effectiveness of both parts of your immune system—no matter how strong it is. Let’s look at some of those complicating factors.
Blood Type
According to a study published in the Annals of Internal Medicine, people with type O and rhesus negative (Rh-) blood groups may have a lower risk of severe coronavirus disease as a result of contracting COVID-19. 3 Ray JG, Schull MJ, Vermuelen MJ, Park A. “Association between ABO and Rh blood groups and SARS-CoV-2 infection or severe COVID-19 illness.” Ann Intern Med. Published online November 24, 2020. All other blood types are at higher risk.
The differences in outcomes between the various blood types were not huge, but they were statistically significant. And as I have been saying repeatedly over the last year, small percentages applied to exceptionally large numbers (the entire population of the world when it comes to COVID), still works out to very large numbers.
DNA
A recent genetic association study identified a gene cluster on chromosome 3 as a risk locus for respiratory failure after infection with COVID-19. This cluster is the major genetic risk factor for severe symptoms after infection and hospitalization. 4 Zeberg H, Pääbo S. “The major genetic risk factor for severe COVID-19 is inherited from Neanderthals.” Nature. 2020 Nov;587(7835):610-612.
The bottom line is that if you have the wrong blood type and the wrong DNA, you are at serious risk of having a bad time with COVID no matter how strong your innate immune system is.
Autoantibodies
 Now, here is a fascinating complicating factor. Laboratory studies suggest that the normal interferon response is suppressed in some people after infection with SARS-CoV-2 (the virus that causes COVID-19), possibly as a result of the virus itself. 5 “NIH clinical trial testing remdesivir plus interferon beta-1a for COVID-19 treatment begins.” NIH News Release. August 6, 2020. (Accessed 22 Jan 2021.) This is important because interferon is your body’s first line of defense against infection.
Now, here is a fascinating complicating factor. Laboratory studies suggest that the normal interferon response is suppressed in some people after infection with SARS-CoV-2 (the virus that causes COVID-19), possibly as a result of the virus itself. 5 “NIH clinical trial testing remdesivir plus interferon beta-1a for COVID-19 treatment begins.” NIH News Release. August 6, 2020. (Accessed 22 Jan 2021.) This is important because interferon is your body’s first line of defense against infection.
In addition, another study published in the October 23, 2020 issue of Science found that 10 percent of patients (mostly men) who developed life-threatening pneumonia as a result of their COVID-19 infection had antibodies that disabled their interferons. 6 Bastard P, Rosen LB, Zhang Q, Michailidis E, et al. “Autoantibodies against type I IFNs in patients with life-threatening COVID-19.” Science. 2020 Oct 23;370(6515):eabd4585. These antibodies—known as autoantibodies, because they attack the body itself—were not found at all in 663 people with mild or asymptomatic Covid-19 infections. And they were found in only 4 of 1,227 healthy patients.
In a second Science study by the same team, the authors found that an additional 3.5 percent of critically ill patients had mutations in genes that control the interferons involved in fighting viruses.7 Zhang Q, Bastard P, Liu Z, et al. “Inborn errors of type I IFN immunity in patients with life-threatening COVID-19.” Science. 2020 Oct 23;370(6515):eabd4570. Given that the body has 500 to 600 of those genes, it is possible that researchers will find even more mutations, said Qian Zhang, lead author of the second study.
Again, interferons are the body’s first line of defense against infection. It is interferons that activate your innate immune system. If interferons are suppressed, your immune system will not respond quickly or even properly no matter how “strong” it is.
The Bradykinin Storm
According to a study from researchers at the Oak Ridge National Laboratory in Tennessee that was published in the science journal eLife last July, patients with severe COVID-19 may experience what is known as a “bradykinin storm.” Bradykinin is a peptide (a biochemical halfway between an amino acid and a protein) that regulates blood pressure.8 Garvin MR, Alvarez C, Miller JI, Prates ET, Walker AM, Amos BK, Mast AE, Justice A, Aronow B, Jacobson D. “A mechanistic model and therapeutic interventions for COVID-19 involving a RAS-mediated bradykinin storm.” Elife. 2020 Jul 7;9:e59177. The researchers found that some people with the coronavirus may produce it in extreme excess. That storm throws major systems—including respiratory, gastrointestinal, and neurological pathways—off balance. This would explain why COVID-19 can lead to blood clots, leaky capillaries, and inflamed blood vessels, which is why some patients may experience heart damage or stroke.
If true, that would make supplementation with antioxidants such as N-acetyl cysteine and systemic proteolytic enzymes such as Seaprose-S and bromelain potentially useful in controlling such a storm because of their peptidase activity. Specifically, we are talking about their ability to both inhibit bradykinin activity as well as lower serum levels of bradykinin.9 Greene EL, Velarde V, Jaffa AA. “Role of reactive oxygen species in bradykinin-induced mitogen-activated protein kinase and c-fos induction in vascular cells.” Hypertension. 2000 Apr;35(4):942-7. , 10 BARBERA S ET AL: “Multicentre clinical study on seaprose S in acute and chronic respiratory inflammation”, MINERVA PNEUMOLOGICA 199612 IT, vol. 35, no. 4, December 1996 (1996-12-01), pages 149 – 156, XP008121030, ISSN: 0026-4954 , 11 Lotz-Winter H. “On the pharmacology of bromelain: an update with special regard to animal studies on dose-dependent effects”. Planta Med. 1990 Jun;56(3):249-53.
The bottom line is that if you have the wrong blood type, the wrong DNA, autoantibodies, or are deficient in systemic proteolytic enzymes and NAC, you are at serious risk of having a bad time with COVID, again, no matter how strong your innate immune system is. Yes, a good immune system is important, but in this case bad luck trumps a good immune system. If you are in that position, you either need to be immune to the virus in the first place or have a supply of natural antipathogens on hand to crush it from the get-go so your bad luck conditions never come into play. Otherwise, you are looking at a stay in the hospital no matter how strong your innate immune system might be. And a stay in the hospital should never be your first option.
COVID-19 Mutations
 Last May, I mentioned that a complication when it comes to vaccines is mutation. A vaccine developed to combat one strain of COVID-19 may not be as effective when confronting a different strain, and the coronavirus has already shown an ability to mutate. The flu is an example of a virus that constantly mutates. To be sure, many mutations in a virus lead to no discernible changes in how it behaves. However, some changes in the genetic structure can lead to changes in how infectious the virus is, how deadly it is, or even how it responds to existing vaccines. With that in mind, 13 mutations have already been identified in the COVID virus, and one of those new strains, the UK strain, is on its way to becoming dominant worldwide and appears to be more contagious. If not more deadly, than the versions that spread in the early days of the COVID-19 pandemic.
Last May, I mentioned that a complication when it comes to vaccines is mutation. A vaccine developed to combat one strain of COVID-19 may not be as effective when confronting a different strain, and the coronavirus has already shown an ability to mutate. The flu is an example of a virus that constantly mutates. To be sure, many mutations in a virus lead to no discernible changes in how it behaves. However, some changes in the genetic structure can lead to changes in how infectious the virus is, how deadly it is, or even how it responds to existing vaccines. With that in mind, 13 mutations have already been identified in the COVID virus, and one of those new strains, the UK strain, is on its way to becoming dominant worldwide and appears to be more contagious. If not more deadly, than the versions that spread in the early days of the COVID-19 pandemic.
Now, so far, the scientific community says that the existing vaccines will work just fine when used directly against the mutations they’ve seen. But there is a hole in those comforting words. You see, a vaccine’s efficacy can be affected indirectly too.
The strains of COVID that you have probably heard about so far are the original Chinese strain (what President Trump liked to call the Wuhan virus), the European strain (which is the strain that developed in Europe as the virus mutated there and which became the strain that first infected the U.S.), and the UK variant (which first appeared in the UK this fall and is rapidly becoming the dominant strain in the U.S.). Other strains such as the South African, Danish, and Brazilian variants have also appeared. For the moment, though, let’s focus on the UK strain.
As a quick summary, it is no deadlier than the previous strains, and experts tell us the current crop of vaccines will work just fine against it. So, what is the problem? Well, first of all, although it is no more deadly, it is twice as infectious. This means it will spread faster and infect more people in a shorter time. Given the same mortality rate but applied to a greater number of people becoming infected, this obviously means that more people will die in the short term, which we now are seeing. But how does this affect the vaccines’ efficacy.
As it turns out, in two ways.
More People Infected Means More Mutated Strains
As we know from our experience with cancer, every time a cell divides, the DNA in it is transcribed or copied from one cell to the next. It is the central miracle of life. Considering that the human genome contains billions of pieces of information, the process of copying is remarkably accurate. But “remarkably” is not the same as “perfectly”. Every time DNA is copied, there are a tiny number of errors. As with a virus, the overwhelming number of these errors are insignificant, at least in the short term. Only a tiny percentage of these very few errors are of any consequence.
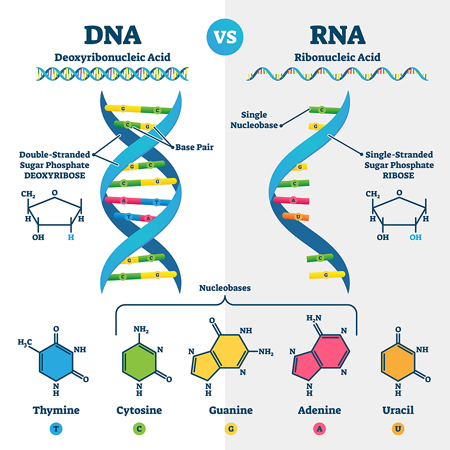
So, what does this have to do with the COVID virus, given that the COVID virus doesn’t even contain any DNA, just RNA? (Most viruses are RNA coded, although some use DNA coding.)
DNA and RNA are similar, although DNA is a double-stranded molecule, whereas RNA is a single-stranded molecule. RNA is essentially a temporary copy of a short segment of DNA. Now, as I just mentioned, COVID is an RNA virus. That is to say, the genetic material for SARS-CoV-2 is encoded in RNA, not DNA. The RNA coding of a virus is orders of magnitude less complex than human DNA, which means that replication errors occur far less frequently than in human DNA. But again, less does not mean zero, and, once again, small percentages applied to large numbers still equals large numbers.
So, again, what does this have to do with us? Well, quite simply, the COVID virus invades cells in our body and then hijacks the DNA replicating “hardware” in the cell’s nucleus to now produce upwards of 105 new RNA encoded virions. Ultimately, at the height of infection, we are talking about your body containing upwards of 109-1010 (i.e., one-10 billion) virions. So, now you’re talking about a low probability of a significant mutation for any one replication being multiplied by a factor of 10 billion.
As stated in the academic journal, The Conversation, “Based on current data, it seems as though SARS-CoV-2 mutates much more slowly than the seasonal flu.12 Niema Moshiri. “Here’s how scientists are tracking the genetic evolution of COVID-19.” The Conversation. April 6, 2020. (Accessed 26 Jan 2021.) Specifically, SARS-CoV-2 seems to have a mutation rate of less than 25 mutations per year, whereas the seasonal flu has a mutation rate of almost 50 mutations per year. And in fact, this is exactly what we are seeing with the COVID virus producing somewhere between 13-17 variants through December 31st—but with only about three to five of those variants having been identified as functionally significant in that they are more infectious.
So, how does this affect vaccines? Well, the UK variant has double the infection rate of the European and Chinese variants. And if you double the infection rate, you double the speed at which the virus spreads. And if you double the number of people infected, you double the number of opportunities for mutation. And if you double the number of mutations, you ultimately double the chances of producing a mutation that is either deadlier or resistant to the vaccine.
Double the Infectiousness of the Virus and You Drive Up the Numbers Required for Herd Immunity
As I explained last May, how quickly a virus spreads is determined by its effective reproduction number, or R0 (R naught). Simply explained, R0 represents the average number of people infected by one infectious individual. If R0 is larger than 1, the number of infected people will likely increase exponentially. The thing is that herd immunity is directly tied to R0.
To achieve herd immunity, you need to make sure that at least a proportion of 1–1/R0 of the population is immune. For the original European coronavirus with an R0 of 2.5, this means that we needed to get at least a proportion of 1–1/2.5=0.6 of the population immune. The 0.6 result in the equation means that at least 60% of the population needs to be immune for herd immunity to kick in. But for the UK variant that appears to have an R0 value of 3.2 or higher, that works out to 1–1/3.2=0.69, which translates to at least 69% needing to be immune. And with 30% of the U.S. population currently saying they do not intend to get vaccinated (plus those who intend to but don’t), that presents a problem.
Then There Are the South African and Brazilian Variants
Researchers identified a new variant in South Africa in late 2020. This variant has spread rapidly across South Africa and into other countries1. It carries many mutations in the SARS-CoV-2 spike protein—the immune system’s prime target, which allows the virus to identify and infect host cells—including some changes linked to weakened antibody activity against the virus. To translate, there is at least some indication that the current crop of vaccines may not be as effective against this variant—although initial indications are that any change in efficacy would be moderate. And as with the UK variant, the new South African variant appears to be more contagious, which is a problem because tougher restrictions may be needed to control the spread.
Whether these mutations in the spike protein could lessen the effectiveness of vaccines is still uncertain. But if not this variant, eventually a variant is coming down the pike that will bypass the current crop of vaccines. Perhaps the Danish variant which carries three mutations in the spike protein which could interfere with the vaccines’ efficacy might present a problem for the vaccines. According to Barbara Ferrer, the Los Angeles Public Health Director, “Current projections by the experts predict that if left unchecked, this variant could dominate locally by March.” And now, there is a Brazilian variant, which also has mutations in the spike protein.
The American Variant
Since the U.S. has had, by far, the most cases of COVID of any country in the world—two and half times as many as second place India, and since virus mutations are statistically a function of the number of cases, it is almost guaranteed that the U.S. has already generated multiple variants on its own. But remember, most variants are not functionally significant, so that could be true of all the variants created in the U.S. so far. On the other hand, there could be significant homegrown variant(s) that we do not know about. How could that be? Quite simply, and quite embarrassingly, the U.S. ranks 43rd among all countries in the world when it comes to coronavirus genome sequencing.13 Harry Stevens and Miriam Berger “U.S. ranks 43rd worldwide in sequencing to check for coronavirus variants like the one found in the U.K.” The Washington Post. Dec. 23, 2020. (Accessed 27 Jan 2021.) Bottom line: when it comes to American variants, at least to this point in time, we are flying blind.
Variants Going Forward
In fact, new variants threatening to bypass the vaccines are likely to be a regular occurrence over time. We are possibly even talking about annual variants resistant to existing vaccines as with the flu virus. If so, new versions of the COVID vaccine (or booster shots for the existing vaccines) will regularly need to be developed and deployed to keep the virus in check, which is pretty much what I predicted last February.
In fact, on January 13th, the CEO of COVID-19 vaccine maker Moderna warned that the COVID-19 will become endemic, saying “SARS-CoV-2 is not going away. We are going to live with this virus, we think, forever.”14 Berkeley Lovelace Jr. “Moderna CEO says the world will have to live with Covid ‘forever’.” CNBC Jan 13 2021. (Accesed 21 Jan 2021.)
He went on to say, “Health officials will have to continuously watch for new variants of the virus, so scientists can produce vaccines to fight them.”
And of course, these new variants are just as likely to be problematic for those counting on their own immune system handling the problem. Just think about it for a moment. Variants that can bypass the vaccines are just as likely to bypass any antibodies you have developed as a result of being infected by earlier variants.
The one positive piece of news here is that, over time, as we keep developing resistance to more and more variants, the symptoms of any COVID infection we get from any new variants are likely to get less and less. Down the road some years, a COVID infection will be much like a flu infection or a bad cold.
So, What Can We Look Forward To?
 Right now, the virus has a head of steam, and new, more contagious strains are becoming dominant. The next two to three months are about to be extremely unpleasant—outside of nursing homes, surprisingly, since that is where the first vaccinations are being concentrated. That alone, will likely prevent mortality statistics from climbing much higher on a daily basis. But although the mortality statistics will look better at first glance, things will be worse for those outside nursing homes. And even though the number of deaths each day will stabilize, or even drop slightly, the numbers of people who experience long-term symptoms will continue to soar.
Right now, the virus has a head of steam, and new, more contagious strains are becoming dominant. The next two to three months are about to be extremely unpleasant—outside of nursing homes, surprisingly, since that is where the first vaccinations are being concentrated. That alone, will likely prevent mortality statistics from climbing much higher on a daily basis. But although the mortality statistics will look better at first glance, things will be worse for those outside nursing homes. And even though the number of deaths each day will stabilize, or even drop slightly, the numbers of people who experience long-term symptoms will continue to soar.
I have been telling you for months that, although largely undocumented, the number of people infected with COVID-19 who developed long-haul symptoms was in the range of 10-20%. Well, it turns out that I was not exaggerating those numbers; in fact, I was underestimating them. Documented statistics are now starting to appear worldwide and from the CDC, the NIH, and the AMA. And they are saying with certainty that the number of patients experiencing long-term chronic symptoms including shortness of breath, chronic fatigue, muscle aches, dysautonomia (a dysfunction of the nerves that regulate nonvoluntary body functions, such as heart rate, blood pressure, and sweating), sleep disturbances, and brain fog are actually running at a truly frightening 25% to 35% of all post COVID patients.15 Len Strazewski. “Dr. Fauci offers 2021 forecast on COVID-19 vaccines, treatments.” AMA Nov 9, 2020. (Accessed 23 Jan 2021.) And even among asymptomatic patients, about 60% have some indication of heart inflammation.16 Strazewski. Make no mistake; this is a big deal. What this means is that 25-60% of you who get COVID, even if you do not die, and no matter how mild the symptoms you experience, are likely to be compromised to some degree for weeks, months, or even years. Again, it really is a big deal.
If you’re not going to get vaccinated, then you’re going to need a strategy to stop it in its tracks if you do get infected by the virus. Denial is not a strategy.
COVID and the Brain, a Very Disturbing Study
 And while we’re on the subject of long-term neurological side effects associated with COVID, an extremely disturbing study was just published on January 19, 2021 in the journal Viruses.17 Kumari P, Rothan HA, Natekar JP, Stone S, Pathak H, Strate PG, Arora K, Brinton MA, Kumar M. “Neuroinvasion and Encephalitis Following Intranasal Inoculation of SARS-CoV-2 in K18-hACE2 Mice.” Viruses. 2021 Jan 19;13(1):132. And while it is a study using mice, there is enough corroboration to be found in all the neurological side effects in humans that makes it likely it applies to us as well.
And while we’re on the subject of long-term neurological side effects associated with COVID, an extremely disturbing study was just published on January 19, 2021 in the journal Viruses.17 Kumari P, Rothan HA, Natekar JP, Stone S, Pathak H, Strate PG, Arora K, Brinton MA, Kumar M. “Neuroinvasion and Encephalitis Following Intranasal Inoculation of SARS-CoV-2 in K18-hACE2 Mice.” Viruses. 2021 Jan 19;13(1):132. And while it is a study using mice, there is enough corroboration to be found in all the neurological side effects in humans that makes it likely it applies to us as well.
The key findings of the study were, not surprisingly, that three days after the mice were infected with the SARS-CoV-2, they displayed high levels of virus in their lungs. But by days five and six, things started to get interesting. Again, not surprisingly, their lungs had started to clear up, but their brains showed almost 1,000-fold more virus than the peak levels found in the lungs. That coincided with the arrival of severe symptoms such as labored breathing, disorientation, and weakness.
The virus also triggered an inflammatory response in the brain, marked by the release of cytokines. As we have discussed numerous times when exploring cytokine storms, too many cytokines tell the body to attack its own cells, triggering dangerous levels of inflammation. The brains of the mice in the study showed around 10 to 50 times more cytokines than the peak levels found in the lungs.
To quote from the study:
In the brain, no increase in the mRNAs of the cytokines or chemokines tested was observed on day 1 after infection. Less than a 10-fold increase was observed in the cytokine mRNA levels on day 3 (Figure 4C). There was a 500-fold increase in IL-6 mRNA by day 5 after infection. TNF-α and IFN-γ mRNA levels increased by ~ 750-fold in the brain by day 5 after infection. Similarly, IL-1β mRNA levels increased by 400-fold by day 5 after infection. Both CCL2 and CCL3 mRNA levels were elevated by almost 1000-fold on days 5 and 6 after infection consistent with the high level of virus in the brain (Figure 4D). These results indicate that the inflammatory response was more pronounced in the brain than in the lungs at the later stage of infection.
In some mice, the reaction caused immediate death. But in mice with milder cases, the virus seemed to hide out in the brain indefinitely.
So again, if the coronavirus is a hoax, it is an extremely nasty hoax with real world consequences far beyond any other hoax I have ever seen.
Down the Road
 Whatever help the vaccines provide is still down the road for most of us, even if you want to get it. And for those looking for a return to normal, I think that is unlikely for the foreseeable future. Yes, as more people get vaccinated, things will back down somewhat, but they will be nowhere near gone. We will be nowhere near normal. Too many people are going to refuse to get vaccinated to reach herd immunity. We are going to be looking at masks and social distancing well beyond this coming fall. And as people continue to ignore those guidelines, we will also be looking at occasional lock downs. Also, in a blow to the strategy of relying on “natural” infection to achieve herd immunity, previous infection with the coronavirus seems to offer little protection against the South African variant. As Alex Sigal, a virologist at the Africa Health Research Institute, says, “We have reason to be concerned because the virus has found a way to escape from previous antibodies.” 18 Tim Cocks, Alexander Winning. “Previous coronavirus infection may offer less protection from new variant.” Reuters. January 18, 2021. (Accessed 28 Jan 2021.) In this regard, vaccines may offer both stronger and longer lasting resistance to infection than natural immunity, especially if the initial natural infection was either mild of asymptomatic.
Whatever help the vaccines provide is still down the road for most of us, even if you want to get it. And for those looking for a return to normal, I think that is unlikely for the foreseeable future. Yes, as more people get vaccinated, things will back down somewhat, but they will be nowhere near gone. We will be nowhere near normal. Too many people are going to refuse to get vaccinated to reach herd immunity. We are going to be looking at masks and social distancing well beyond this coming fall. And as people continue to ignore those guidelines, we will also be looking at occasional lock downs. Also, in a blow to the strategy of relying on “natural” infection to achieve herd immunity, previous infection with the coronavirus seems to offer little protection against the South African variant. As Alex Sigal, a virologist at the Africa Health Research Institute, says, “We have reason to be concerned because the virus has found a way to escape from previous antibodies.” 18 Tim Cocks, Alexander Winning. “Previous coronavirus infection may offer less protection from new variant.” Reuters. January 18, 2021. (Accessed 28 Jan 2021.) In this regard, vaccines may offer both stronger and longer lasting resistance to infection than natural immunity, especially if the initial natural infection was either mild of asymptomatic.
Also, an issue with intramuscular vaccines is that they are not very good at migrating from the bloodstream to the nasal mucosa. In other words, the vaccine might prevent you from getting sick but still allow the virus to bloom in your nose—from where it could then easily spread to other people.
A quote from Michal Tal, an immunologist at Stanford University, gives a hint as to what this might mean in regard to what the new normal might look like.19 Apoorva Mandavilli. “Here’s Why Vaccinated People Still Need to Wear a Mask.” The New York Times. Dec. 8, 2020. (Accessed 29 Jan 2020.)
The new vaccines will probably prevent you from getting sick with Covid. No one knows yet whether they will keep you from spreading the virus to others…A lot of people are thinking that once they get vaccinated, they’re not going to have to wear masks anymore. It’s really going to be critical for them to know if they have to keep wearing masks, because they could still be contagious.
And then there are the virus mutations that will appear down the road—some of which will be vaccine and immune system resistant. So, once again as I stated last February and as the CEO of Moderna stated just a few days ago, it looks like COVID is with us, at least in some form and at some level, for the foreseeable future.
So, a question that I keep getting asked is: “Am I personally planning to get vaccinated.” And the answer is “yes.” Now, don’t get me wrong, it’s not because I’m concerned about getting the virus (I believe I already had it last March). Nor am I concerned about lingering side effects if I do get it again. I have full confidence in the ability of my antipathogen formula to handle it easily, quickly, and without any lingering issues if I do get it a second time—as it did when I contracted it the first time. No, the reasons I would get vaccinated are:
- It’s important to walk your talk. If I’m asserting that the COVID vaccines are mostly safe, then I should be willing to get vaccinated myself.
- The more people who get vaccinated, the sooner herd immunity will be reached, which will protect even those who don’t get vaccinated.
- And it is becoming obvious that as things move forward, and despite scientific, ethical, and even legal issues, having proof of vaccination (an immunity passport) will be mandatory to engage in many activities, including the ability to use your passport and travel outside the country.20 Brown RCH, Kelly D, Wilkinson D, Savulescu J. “The scientific and ethical feasibility of immunity passports“. Lancet Infect Dis. 2020 Oct 16:S1473-3099(20)30766-0.
That said, because I have a good supply of Super ViraGon and Immunify at home, I feel no pressure to rush out and get vaccinated. I am quite comfortable letting all those at much greater risk get their shots first. Also, it does not hurt that the hours-long wait to make an appointment and get vaccinated is likely to disappear in the next couple of months, I’m guessing it will all be much faster and easier by mid-summer, which is when I’ll look to get vaccinated.
An Update on the Closing of Baseline Nutritionals
And speaking of my antipathogen formula, as most of you already know, Baseline Nutritionals, the only place you can buy that formula, is in the process of closing its doors (although we are still looking for a company of sufficient size, experience, and quality to acquire it). 17 of the company’s 24 formulas are already sold out. And of the 7 left, some will be gone in the next few days. There is a reasonable supply of the Super ViraGon still available, but it is unlikely to last until the end of March. And if there is any surge in buying, it might not see the end of February. Bottom line: if you are thinking of stocking up, you might want to do it sooner rather than later.
By the way, for any of you who think this might be important, a number of the active biochemicals found in the ingredients in this formula (garlic,21 Song H, Cui J, Mossine VV, Greenlief CM, Fritsche K, Sun GY, Gu Z. “Bioactive components from garlic on brain resiliency against neuroinflammation and neurodegeneration.” Exp Ther Med. 2020 Feb;19(2):1554-1559. zinc,22 Qi Z, Liu KJ. “The interaction of zinc and the blood-brain barrier under physiological and ischemic conditions.” Toxicol Appl Pharmacol. 2019 Feb 1;364:114-119. olive leaf extract,23 Hornedo-Ortega R, Cerezo AB, de Pablos RM, Krisa S, Richard T, García-Parrilla MC, Troncoso AM. “Phenolic Compounds Characteristic of the Mediterranean Diet in Mitigating Microglia-Mediated Neuroinflammation.” Front Cell Neurosci. 2018 Oct 23;12:373. and oil of wild mountain oregano,24 Zhang Y, Long Y, Yu S, Li D, Yang M, Guan Y, Zhang D, Wan J, Liu S, Shi A, Li N, Peng W. “Natural volatile oils derived from herbal medicines: A promising therapy way for treating depressive disorder.” Pharmacol Res. 2020 Dec 11;164:105376. e.g.) have been proven to cross the blood-brain barrier so that they may support the body in eliminating any viruses hiding there as well as reduce any brain inflammation.
Addendum
As predicted above, on January 29th, the discovery a brand new Los Angeles variant was announced. This is the first U.S. variant discovered. But as surely as people don’t like to wear masks, more U.S. variants will be discovered as the level of gene sequencing increases in the U.S., up from its current 43rd position in the world.
References
| ↑1 | “Leading Causes of Death.” CDC National Center for Disease Control. October 30, 2020. (Accessed 18 Jan 2021.) |
|---|---|
| ↑2 | Jake Lahut “Ex-GOP pollster Frank Luntz says ‘I don’t want to do this anymore’ after ‘unity’ themed focus group goes off the rails.” Business Insider. 21 Jan 2021. (Accessed 21 Jan 2021.) |
| ↑3 | Ray JG, Schull MJ, Vermuelen MJ, Park A. “Association between ABO and Rh blood groups and SARS-CoV-2 infection or severe COVID-19 illness.” Ann Intern Med. Published online November 24, 2020. |
| ↑4 | Zeberg H, Pääbo S. “The major genetic risk factor for severe COVID-19 is inherited from Neanderthals.” Nature. 2020 Nov;587(7835):610-612. |
| ↑5 | “NIH clinical trial testing remdesivir plus interferon beta-1a for COVID-19 treatment begins.” NIH News Release. August 6, 2020. (Accessed 22 Jan 2021.) |
| ↑6 | Bastard P, Rosen LB, Zhang Q, Michailidis E, et al. “Autoantibodies against type I IFNs in patients with life-threatening COVID-19.” Science. 2020 Oct 23;370(6515):eabd4585. |
| ↑7 | Zhang Q, Bastard P, Liu Z, et al. “Inborn errors of type I IFN immunity in patients with life-threatening COVID-19.” Science. 2020 Oct 23;370(6515):eabd4570. |
| ↑8 | Garvin MR, Alvarez C, Miller JI, Prates ET, Walker AM, Amos BK, Mast AE, Justice A, Aronow B, Jacobson D. “A mechanistic model and therapeutic interventions for COVID-19 involving a RAS-mediated bradykinin storm.” Elife. 2020 Jul 7;9:e59177. |
| ↑9 | Greene EL, Velarde V, Jaffa AA. “Role of reactive oxygen species in bradykinin-induced mitogen-activated protein kinase and c-fos induction in vascular cells.” Hypertension. 2000 Apr;35(4):942-7. |
| ↑10 | BARBERA S ET AL: “Multicentre clinical study on seaprose S in acute and chronic respiratory inflammation”, MINERVA PNEUMOLOGICA 199612 IT, vol. 35, no. 4, December 1996 (1996-12-01), pages 149 – 156, XP008121030, ISSN: 0026-4954 |
| ↑11 | Lotz-Winter H. “On the pharmacology of bromelain: an update with special regard to animal studies on dose-dependent effects”. Planta Med. 1990 Jun;56(3):249-53. |
| ↑12 | Niema Moshiri. “Here’s how scientists are tracking the genetic evolution of COVID-19.” The Conversation. April 6, 2020. (Accessed 26 Jan 2021.) |
| ↑13 | Harry Stevens and Miriam Berger “U.S. ranks 43rd worldwide in sequencing to check for coronavirus variants like the one found in the U.K.” The Washington Post. Dec. 23, 2020. (Accessed 27 Jan 2021.) |
| ↑14 | Berkeley Lovelace Jr. “Moderna CEO says the world will have to live with Covid ‘forever’.” CNBC Jan 13 2021. (Accesed 21 Jan 2021.) |
| ↑15 | Len Strazewski. “Dr. Fauci offers 2021 forecast on COVID-19 vaccines, treatments.” AMA Nov 9, 2020. (Accessed 23 Jan 2021.) |
| ↑16 | Strazewski. |
| ↑17 | Kumari P, Rothan HA, Natekar JP, Stone S, Pathak H, Strate PG, Arora K, Brinton MA, Kumar M. “Neuroinvasion and Encephalitis Following Intranasal Inoculation of SARS-CoV-2 in K18-hACE2 Mice.” Viruses. 2021 Jan 19;13(1):132. |
| ↑18 | Tim Cocks, Alexander Winning. “Previous coronavirus infection may offer less protection from new variant.” Reuters. January 18, 2021. (Accessed 28 Jan 2021.) |
| ↑19 | Apoorva Mandavilli. “Here’s Why Vaccinated People Still Need to Wear a Mask.” The New York Times. Dec. 8, 2020. (Accessed 29 Jan 2020.) |
| ↑20 | Brown RCH, Kelly D, Wilkinson D, Savulescu J. “The scientific and ethical feasibility of immunity passports“. Lancet Infect Dis. 2020 Oct 16:S1473-3099(20)30766-0. |
| ↑21 | Song H, Cui J, Mossine VV, Greenlief CM, Fritsche K, Sun GY, Gu Z. “Bioactive components from garlic on brain resiliency against neuroinflammation and neurodegeneration.” Exp Ther Med. 2020 Feb;19(2):1554-1559. |
| ↑22 | Qi Z, Liu KJ. “The interaction of zinc and the blood-brain barrier under physiological and ischemic conditions.” Toxicol Appl Pharmacol. 2019 Feb 1;364:114-119. |
| ↑23 | Hornedo-Ortega R, Cerezo AB, de Pablos RM, Krisa S, Richard T, García-Parrilla MC, Troncoso AM. “Phenolic Compounds Characteristic of the Mediterranean Diet in Mitigating Microglia-Mediated Neuroinflammation.” Front Cell Neurosci. 2018 Oct 23;12:373. |
| ↑24 | Zhang Y, Long Y, Yu S, Li D, Yang M, Guan Y, Zhang D, Wan J, Liu S, Shi A, Li N, Peng W. “Natural volatile oils derived from herbal medicines: A promising therapy way for treating depressive disorder.” Pharmacol Res. 2020 Dec 11;164:105376. |