
- Understanding pandemics throughout history and what we have learned from them
- What the data really means
- Let’s talk about masks
- The important number that no one is talking about
- Going to school
- Using a natural antipathogen formula as a prophylactic to prevent ever getting the virus
- Looking forward
If you are from a country that has the coronavirus somewhat under control, then this newsletter is not for you. That said, feel free to read it for entertainment value, but for the most part, it does not apply to you.
Some History
I have had to do a number of rethinks on this newsletter. There were issues relative to the coronavirus that were important to explore, but it has become obvious, especially since the last newsletter, that we have reached the limits of science-based arguments supported by studies. It turns out that bad information is even more contagious than the coronavirus, and there is no way to counter it. Science is no longer an effective counter when so many people choose to believe scientists are lying to them and opt instead to believe in the most extreme theories circulating on the internet. When it comes to COVID-19, people have staked out their territory and pitched their camps based on their beliefs. There are those who automatically believe what scientists and medical experts tell us about the virus–even when they are repeatedly shown to be wrong. On the other hand, there are those who choose to disbelieve the mainstream scientific community and choose to follow the advice of more fringe “experts,” even when those experts also tell us that people are getting sick because they have sex with astral demons in their sleep and that vaccines are dangerous because they are made with alien DNA (and no, I am not talking about the aliens who come to the United States by migrating across the border).
I was planning to do my usual thing and write a newsletter filled with citations and scientific references, but things have changed so much in the last three months. For a huge swath of the public, science no longer works as an explanation for what’s happening with the coronavirus. People are looking for a bigger, grander, more all-encompassing explanation for the chaos we now face–an explanation far beyond the reach of science.
So, a different approach is required. Instead of arguing the science, let me present a narrative that might inform how we look at the facts on the ground. And the best place to begin is with a little history about pandemics. This also happens to be a freebie for me since I can cut and paste from the section on pandemics that I just put together for the rewrite of Lessons from the Miracle Doctors. Incidentally for those of you who are interested, I have now finished 28 of what will be 30 chapters in the book. With just two chapters to go, the book is now over 350,000 words and has over 1700 clickable citations. I expect to finish by the end of August at which point I will turn it over to the editors for proofing and formatting for Kindle and Apple Books, etc., which will likely take 2-3 months. But enough about me.
Pandemics
Let’s take a quick look at some of the great pandemics in human history to get a sense of how long they lasted, how many they killed, and how they ended.
Plague of Justinian (Bubonic plague)
- Lasted 200 years (The bulk of the deaths occurred between 541 and 542, but this pandemic was stubborn and did not fade entirely until 750.)
- Killed upwards of half the world’s population
- Ended when there was no one left to infect. Half the world had died, and the other half had been infected, survived, and was now immune.
Black Death
- The bubonic plague returned to Europe in 1347. It lasted on and off for about 300 years.
- In just four years, it killed half the population of Europe. The plague resurfaced roughly every 20 years from 1348 to 1665–40 outbreaks in 300 years. And with each new plague epidemic, 20 percent of the men, women, and children living in London were killed.
- It ended essentially by locking away the sick so they could not infect the healthy and by burying the dead in mass graves.
Smallpox in the New World
- Smallpox was endemic to Europe, Asia, and Arabia for centuries. It killed 30% of all those infected and left survivors with pockmarked faces. It was carried to the New World in the 15th century with the first European explorers. The indigenous populations had zero resistance. To them, it was a “novel” virus.
- Over the next hundred years, it wiped out 90-95% of the native population. In Mexico, the population dropped from 11 million pre-conquest to just one million. Smallpox in the New World is far and away the deadliest pandemic in human history.
- It ended when there were no more native Americans left to infect.
- The smallpox vaccine, introduced by Edward Jenner in 1796, was the first successful vaccine to ever be developed. It took 200 years of vaccinations to eradicate smallpox. In 1980, the World Health Assembly declared smallpox eradicated. No cases of naturally occurring smallpox have happened since. Other pathogens such as bubonic plague have had ebbs and flows throughout history, but smallpox is the only pathogen, so far, that has ever been eliminated from the face of the earth!
- We came close with polio, but fear of vaccination in a handful of countries in Africa and Asia is causing the number of cases to increase. One disturbing thought is that if the disease breaks out of the handful of countries in which it is now contained, no one in the developed world any longer has any immunity to the disease. It would spread rapidly.

Cholera
- Cholera originated in the Ganges delta in India.
- During the 19th century, it spread across the world. Six subsequent cholera pandemics have killed millions of people across all continents. The current (seventh) pandemic started in South Asia in 1961 and reached Africa in 1971 and the Americas in 1991. It is still active.
- In the mid-19th century, cholera killed tens of thousands in London. John Snow, a British Doctor figured out that it was being transmitted by contaminated water. Specifically, people were being infected by drinking water contaminated by sewage flowing near the infected wells.1 Kathleen Tuthill. “John Snow and the Broad Street Pump.” UCLA Department of Epidemiology. Nov 2003. (Accessed 20 Jul 2020. https://www.ph.ucla.edu/epi/snow/snowcricketarticle.html) Improving urban sanitation in the developed world led to an end of cholera pandemics in the developed world. Unfortunately, it is still a persistent killer in third-world countries lacking adequate sewage treatment and access to clean drinking water.
HIV/AIDS: Sub Saharan Africa
- 1981 to the present.
- Between 56 and 100 million people have become infected with HIV since the start of the pandemic.2 “Global HIV & AIDS statistics–2020 fact sheet.” UNAIDS. (Accessed 20 Jul 2020.) https://www.unaids.org/en/resources/fact-sheet. (Note: WHO actually defines HIV as a “global epidemic,” whatever that means. And between 25 and 42 million people have died from AIDS-related illnesses since the start of the epidemic.
- It is far from gone, but HIV can be well managed in the developed nations so it doesn’t progress to AIDS. Nevertheless, AIDS is still incredibly deadly in developing nations without access to adequate health care and preventative measures.
Spanish Flu
- A number of deadly flu outbreaks have occurred over the years, but the 1918 Spanish flu is the worst in history. Although called the Spanish Flu, scientists are mostly sure it didn’t start there. Best guess is that it originated in the United States, with China a strong runner up possibility.
- It is estimated that in just two years 500 million people, or one-third of the global population was infected. It is also estimated that 40-50 million died.
- There were no vaccines and no therapeutics. In the end, it disappeared as the result of wearing masks and social distancing.
So, What Have We Learned About Pandemics?
Yes, all pandemics eventually end, at least for a while. But not all pandemics end in a few months like the flu. Many can continue for several hundred years before they seem to “magically disappear”–only to circle back every generation as herd immunity disappears with the next generation, to strike again and again. However, even though we are unable to eliminate most pandemic pathogens, we have several major advantages over the ancients.
- We are much better at understanding how pathogens infect, spread, and kill.
- This allows us to implement policies that inhibit their ability to spread and develop therapeutics that can significantly reduce mortality rates or even help patients live for decades while infected. People infected with HIV can now live mostly symptom free indefinitely. And in the last six years, newly developed therapeutics have dropped the mortality rate for Ebola from 74% to as low as 6% if treated early enough.
- We also have options for testing and contact tracing on a massive scale that were not available to peoples of the past.
- And despite the resistance of many to their use, vaccines of varying efficacy (20% to 90%, with benefits lasting as little as a few months to as long as several decades) and varying side effects (ranging from mild to occasionally deadly) are sometimes available.
As human civilizations have flourished, so too have infectious diseases. It is the inevitable result of large numbers of people living in close proximity to each other–and to animals–often with poor sanitation and nutrition. This provides fertile breeding grounds for disease. In ancient times, overseas and land-based trading routes slowly spread novel infections from country to country, creating the first global pandemics. Today, it is international air travel which can spread a pandemic to opposite ends of the world in a matter of hours!!
Finally, in order, here is a list of the tools we now have at our disposal for combatting pandemics.
1. Vaccines
A low-risk, effective vaccine is the most efficient way to stop the spread of pandemic. Unfortunately, that is easier said than done. In the entire history of humankind, only one pandemic has ever been wiped from the face of the earth through a vaccine. Every other vaccination program has come up short of that in terms of efficacy and/or lack of harm. Some highly effective vaccines have produced significant harm at various times as they have evolved. Specifically, I am talking about the polio vaccine. Yes, it is now highly effective and close to wiping polio off the face of the earth, but along the way, versions of the vaccine caused both polio and brain cancer in patients until those issues were discovered and resolved. To be clear, neither of those issues are present in current iterations of the vaccine–but they were at one time.
The other problem with vaccines, of course, is convincing people to use them. According to a national survey designed and analyzed by Tufts University’s Research Group on Equity in Health, Wealth, and Civic Engagement, only 57% of Americans say they would get a COVID-19 vaccine if it were available. That is not enough to develop herd immunity.
Of course, when it comes to COVID-19, no vaccine is currently available. We have no idea how effective any vaccine in the pipeline will be. And we have no idea what its side effects might be on the population as a whole. Nevertheless, there is a political imperative to get a vaccine injected into everyone’s arm ASAP–cutting the evaluation time from a standard 18 months to as little as six months. What could possibly go wrong developing a vaccine at warp speed?
2. Testing, quarantine, and contact tracing

This can be highly effective. Countries like South Korea and all of the Nordic countries have used this to great effect during the coronavirus pandemic. If you can quickly test for possible infections, quarantine anyone who tests positive, and then trace and quarantine anyone who was in direct contact with the infected person, you can control a pandemic with minimal inconvenience to the population as a whole. In fact, this method alone has kept the infection rate so low that only 5-10% of citizens in the Nordic countries bother to wear a mask in public settings, a figure that has remained stable since the start of the outbreak.
In the United States, this is no longer an option.
- We were late getting into the testing game.
- We are five months into the pandemic, and we still don’t have adequate testing on a per capita basis.
- Test results for most people take far too long to be useful when it comes to either quarantining or contact tracing.
- Accuracy for many of the tests has been dubious, at least so far.
- Too many citizens in the U.S. consider tracing an invasion of their personal freedom and refuse to cooperate with authorities. And the use of a mandatory phone app that would make contact tracing simple, automatic, and require minimal manpower is a non-starter in the United States for privacy reasons. And to tell the truth, given the government’s track record when it comes to monitoring its citizens and invading privacy, I can’t say I disagree. Nevertheless, for those countries that have used them, these apps have been extremely effective at limiting the spread of the virus without requiring an army of trackers and general lockdowns.
- Even if we wanted to now, we have allowed the pandemic to get so out of control and infect so many people that it would be impossible to implement any kind of effective testing, selective quarantine, and contact tracing program at this stage of the game.
- The President does not like any aspect of testing, quarantines, or contact tracing–so this is likely a non-starter, at least on a national basis, at this time.
3. Social distancing
The idea of American exceptionalism is built into our culture. It has always been linked to the idea of freedom. The identification of the United States as a unique embodiment of liberty in a world overrun by oppression goes back to the American Revolution. It has served us well when it comes to things that benefit from innovation, out of the box thinking, and the entrepreneurial spirit. Think business, science, entertainment, and technological innovation. If we were having a political discussion, I would now launch into a discussion of how it shapes our world view and our relationships with other countries throughout the world, but that is for another day and another writer. The issue for us today is that American exceptionalism also has a downside. It serves as the justification for people to take steps on behalf of their own personal freedom over the wellbeing of society as a whole. Here is a picture of Coney Island on July 4th–no social distancing and not a facemask in sight. What more needs be said?

4. Masks and other PPE
When you have already eliminated vaccines, testing, quarantines, contract tracing, and social distancing as options, masks are the next line of defense. Unfortunately, 30% of Americans say they either sometimes, rarely, or never wear a mask when they leave home. At that rate of noncompliance, the virus will spread rapidly. (We will talk more about masks later.)
5. Lockdowns
Lockdowns are the last line of defense. When people are not following the already mentioned guidelines, you end up issuing orders for entire communities to stay at home and lock down for an indefinite period. Just a few days ago, the President said that “lockdowns do not prevent infection in the future,” and he’s absolutely right. I said the same thing in early March. (Makes you wonder if he’s now reading my newsletters.) Since no one gains immunity while in lockdown, all this approach does is buy you time. Time to prepare hospitals and spread out infections so your medical response is not overwhelmed. But as soon as you lift the lockdown, the pandemic is likely to surge as people burst forth from their homes and break all the rules in an orgy of “liberation.” (See picture above.) Also, mass lockdowns are incredibly disruptive to life, mental wellbeing, employment, and the economy. They are a well that can only be drawn from so many times before people refuse to comply. We are probably already at that point.
6. Natural herd immunity
This is what happens when everything else you have tried has failed. There are three problems with it:
- It can take a long time. It took 200 years for natural immunity to take hold during the Plague of Justinian.
- It can be costly in terms of human life. When smallpox tore through the indigenous peoples of North and South America, over 90% of the population died before the 10% that survived the disease gained herd immunity, along with horrible disfigurement.
- It doesn’t last. People have this nasty habit of creating copies of themselves. The problem is that the copies (often called children) do not share their parents’ immunity, and thus the pandemic can resurface again and again and again. As we saw with the Black Death, the plague resurfaced roughly every 20 years from 1348 to 1665–40 outbreaks in 300 years. And with each new plague epidemic, 20 percent of the men, women, and children living in London were killed.
7. Waiting for the pandemic to magically go away

The belief that pandemics magically go away as part of their natural cycles is mostly not true for two reasons.
- So far, no pandemic has permanently disappeared on its own without human intervention. Many have run for hundreds of years, then disappeared, only to surface again years later. This is mostly the result of fading herd immunity.
- Some, like the flu, appear to magically disappear each summer, only to return again each fall. This is the result of viral mutation that renders any existing herd immunity obsolete.
The only pandemic that has completely disappeared from the face of the earth is smallpox, and that was not the result of magically going away, but as a result of the development of a vaccine.
8. Therapeutics
Therapeutics, essentially, are what we do when we cannot get rid of the pandemic. HIV is a great example. We cannot yet stop the spread of the virus, but through the use of therapeutics, we have been able to turn a certain death sentence into decades of relatively normal life. We have learned to co-exist with the pandemic.
The Data
A major problem we now face is that many people question the numbers they see in the news. They are convinced that the death toll is far less than the numbers shown on TV. According to a July 21st poll, nearly one in three Americans are skeptical of the official death count.3 Margaret Talev. “Axios-Ipsos poll: The skeptics are growing.” AXIOS. Jul 21, 2020. (Accessed 30 Jul 2020.) https://www.axios.com/axios-ipsos-poll-gop-skeptics-growing-deaths-e6ad6be5-c78f-43bb-9230-c39a20c8beb5.html They consider the coronavirus pandemic a hoax. The primary claim is that hospitals are inflating the numbers by claiming that if someone dies of a heart attack but was merely in contact with someone who had COVID-19, the hospital will list it as death by COVID-19 not a heart attack because they get reimbursed more for coronavirus deaths. It also does not help that the President is constantly claiming that if there were less testing, the numbers would be less.
Surprisingly, both these claims are partially true. However, even though they contain an element of truth, the parts that aren’t true make them highly misleading and totally irrelevant.
How the Cause of Death is Determined
Let’s start with how hospitals determine the cause of death. Big surprise, everyone, there is nothing new here. Hospitals do this all the time and have done so for years–and no, not to claim higher reimbursement. It’s very simple; in most cases when someone dies, there are comorbidities. Let me give you a very-common example. Someone gets the flu. It causes inflammation of the lung tissue and weakens their immune system. This opens the door for them to catch pneumonia. The pneumonia inflames their arteries, destabilizing plaque on the arterial wall, which then breaks loose and causes a blockage that leads to a heart attack and death.
So, what does the doctor list on the death certificate: flu, pneumonia, arterial inflammation, plaque, arterial blockage, or heart attack. Guess what: there is a protocol for this. It is called the “underlying cause of death,” which is defined as the disease or injury that initiated the train of events leading directly to death. In this case, the death certificate will list the flu as the underlying cause of death.
And that’s how COVID-19 gets listed as the underlying cause of death regardless of any pre-existing comorbidities–because it initiated the “train of events” that led directly to death. Make sense? There is no inflating of numbers here. It’s how the cause of death has been determined for years.
Now to be clear, there are examples of states and/or hospitals:
- Labeling some deaths as COVID related even when an alternative cause is clearly the more likely underlying cause.
- Labeling every death in which someone tested positive for the virus as a COVID death, even when the actual cause of death was totally unconnected, such as an automobile accident or suicide.
- And sometimes labeling deaths as COVID related even when postmortem testing subsequently showed that the deceased never actually had the coronavirus.
But these appear to be very much the exception and not the rule. That said, these “lapses in judgment” don’t add that many deaths to the tally. Also, it should be remembered that we now know the coronavirus was working its way through the United States for at least two months before we knew it was here. That means that it’s likely that several thousand people died from COVID-19 before we even knew that we should look for it, which means that all of those deaths were assigned to some other underlying cause–most likely the flu–when in fact it was the coronavirus that killed them. In other words, before you say that the number of deaths in the U.S. from the coronavirus are overstated, you need to add those uncounted deaths back into your tally since the official count may, in fact, be understated.
The bottom line is that whatever the exact number may be, we can clearly state in general terms that too many people have died from COVID-19.
The More You Test, the More Cases You Will Find
The President is absolutely right. It is 100% true that the more people you test, the more cases you will find. However, closing your eyes and not seeing cases of coronavirus does not mean they are not there. But more importantly, holding back testing, in addition to allowing the virus to spread much faster and reach far more people because you are flying blind, makes another, even more important, number look much worse: the incidence of mortality.
Let’s make this simple. If you test 1,000 people and 100 test positive for COVID-19 and 10 people die, you are looking at a 10% mortality rate (10 out of the 100 who tested positive). On the other hand, if you had tested 10,000, you would have found ten times as many, or 1,000, who tested positive for the virus. (This is the number the President doesn’t like.) However, deaths have nothing to do with testing. In other words, you would still have the same 10 deaths, which means your mortality rate would drop to a mere 1%. In other words, as increased testing reveals more positives (a Presidential bad), your mortality rate drops (a community good).
To put this in simple terms, holding back testing is a bad idea. Flying blind through a major pandemic is a bad idea.
Even Though Cases Are Soaring, Deaths Are Not
As the incidence of COVID-19 has soared over the last few weeks, the number of deaths each day has not kept pace. There may be several reasons for this.
- Increased testing is catching more cases, which as we just discussed lowers mortality rates ipso facto.
- Increased testing is catching more mild cases.
- Younger people are making up a larger share of the cases now. And although they do die, they die at a lower rate than senior citizens.
- Doctors now have therapeutics such as remdesivir that are proven to lower mortality rates and speed up recovery.
- And the President may be half right yet again. He said that warmer temperatures would make the virus magically go away. Well, warmer temperatures certainly haven’t made the virus go away, but they may have made the virus less virulent. If so, unfortunately, we can look for that benefit to disappear in the fall, which means the mortality rate will once again rise, even if just a little, when temperatures drop. That said, COVID-19 does not appear to be a seasonal virus like the flu. Instead it appears to be much more ocean like–just one continuous series of wave after wave after wave–never really going away.
By the way, speaking of deaths, we’re now getting a partial answer to a question that I asked in my last newsletter: how many deaths per day are we willing to tolerate before everyone in the country says, “Enough is enough?” Well, we have now reached 1,000 per day, and it hasn’t yet triggered that response. So, we now know that whatever that level is, it is going to be substantially higher than 1,000 a day.
Frighteningly, when it comes to COVID-19 in the United States, we may be looking at a frog in the water scenario. I’m talking about how a frog will jump out of boiling water but will allow itself to be boiled alive if the temperature is raised slowly, one degree at a time. If deaths back in March had jumped from one to a thousand a day that month, there would have been panic and a national outcry. But by adding a few deaths every day over five months, we now seem to be accepting a thousand a day as just another fact of life that you live with. And if things keep increasing a little at a time, there is no telling how high that number could go without drawing national outrage.
Masks
Now, let’s talk about masks. Dr. Fauci is now saying you should wear a mask anytime you leave your house, and he’s also recommending that you add goggles, face shields, and gloves to the mix. I understand the intent of the new guidelines: keep things as simple as possible (if you’re out of the house wear a mask) and to maximize protection (use everything.) And yes, more is better but not necessarily that much better. We’re talking about the law of diminishing returns here. And considering how resistant so many people are to wearing a mask in any situation–let alone adding face shields and goggles–I’m guessing these new guidelines will be followed even less religiously than the previous guidelines.
Look, something is going on here, and it transcends political lines. It is visceral, and it is driven by anger.
In the 1918 flu pandemic, there were no vaccines and no effective therapeutics. Lockdowns, social distancing, and masks were the primary defense against the spread of the pandemic. Sound familiar? And of the three–hold onto your hats–masks were the most hated and the most resisted by the public. In places where mask orders were successfully implemented, noncompliance and outright defiance quickly became a problem. It really is true, isn’t it: the more things change, the more they stay the same?
What has changed, though, is the arguments against the use of masks. Back in 1918, things were simple. People didn’t like the way they felt. Workers felt they were too uncomfortable to wear all day. They made “their noses fall asleep.” Today, the arguments against them are much grander.
Let’s quickly deal with them.
- They force you to breathe your own air, depriving you of oxygen, and poisoning your body with carbon dioxide. This is only slightly true. Air takes up space. When you blow up a balloon, as air fills the space, the balloon gets bigger. If the balloon does not get bigger, then no air is going into the balloon. That means that if your mask is not getting bigger, the only place “used” air from your lungs can be stored is in the places between the mask and your face. For soft masks that sit close to the face, there just is not much space for holding of used air to be rebreathed. Hard masks, such as N95’s that protrude from the face will definitely hold some used air in the space where the mask protrudes out from your nose and mouth. But just look at the space; it’s not a lot, but it definitely is some.

- Masks “activate” the virus making it more infectious. Yeah, I don’t really know what to say about this one. It’s not a thing. It’s not real. That’s not the way viruses work.
- Masks hold viruses when you touch them so that you breathe them in later. Not really. Viruses travel on water droplets. If an infected droplet lands on your mask, the water is absorbed by the mask which means the virus now sits on the mask and can only be moved by direct contact, no longer by breathing.
- Masks don’t protect you. Absolutely true. As I said back in February, masks provide little protection to the wearer. What they do is impede the dispersal of water droplets expelled from your lungs whenever you breathe, talk, yell, cough, or sneeze–and thus impede how far the viruses traveling on those droplets can travel. Unimpeded, those droplets can ride moisture droplets from your lungs six feet in a couple of seconds. Impeded by a mask, they only travel about 18 inches. That’s why keeping six feet apart and wearing a mask, works to stop spreading infection.
- They are a violation of personal freedom. They are fine to wear for those who want to wear them, but it should be a personal choice. That would be true if we were talking about protecting the wearer. But we are not. We are talking about protecting others from being infected by you. Saying that wearing a mask should be a personal choice is like saying.
- Drinking and driving should be a personal choice.
- Yelling fire in a theater should be a personal choice.
- Going out to a crowded neighborhood bar while infected with Ebola should be a personal choice.
On the other hand, wearing a mask when it doesn’t accomplish anything–and in fact makes activities more difficult–is questionable and will lead to noncompliance.
- Places to wear a mask:
- Pretty much anyplace indoors outside your own home where other people are present.
- Anyplace outdoors where you cannot keep socially distant.
- Places in which wearing a mask provides only marginal benefit:
- Outdoors in general–as long as you can keep socially distant.
- While exercising outdoors alone, cycling, or running. (Note: when cycling of running, you can leave a slipstream of droplets trailing as much as 27 feet behind you. However, they tend to be so dissipated in the air as to be minimally infectious.)
- Any indoor work situation that significantly increases your breathing rate (in which case your employer will need to allow for 12 feet of social distancing between workers).
Final thought. As we have already discussed, if you have the virus under control with sufficient testing, contact tracing, and social distancing, then very few people out in public are likely to be infected and potentially infecting others, and the need for wearing masks at all is minimal. And as we see in the Nordic countries, very few people wear masks, and they have no problem. Unfortunately, the U.S. is not in that position. In the U.S. masks offer the last line of defense. If enough people in the U.S. choose not to wear masks, we are in for an extended world of hurt.
PS: Since masks tend to reduce droplet travel to about 18 inches, they will not be effective if you can’t also keep socially distant.
William Henry Gates III
Poor Bill Gates. Back in 2011, he was accused by conspiracy theorists within the alternative health community of claiming to want to use vaccines to kill off 1 billion children, which, of course, is not what he said at all…or did.
Now, he is being accused of trying to use COVID-19 medical and dental injections to implant tracking chips. I mentioned this “theory” in my last newsletter and received several strongly worded emails accusing me of being naïve and not understanding the truth behind the accusation. In fact, according to a poll, fully half of all Americans who name Fox News as their primary news source believe the story that Bill Gates is looking to use a coronavirus vaccine to inject a microchip into people and track the world’s population.4 Andrew Romano. “New Yahoo News/YouGov poll shows coronavirus conspiracy theories spreading on the right may hamper vaccine efforts.” Yahoo News. May 22, 2020. (Accessed 31 Jul 2020.) https://news.yahoo.com/new-yahoo-news-you-gov-poll-shows-coronavirus-conspiracy-theories-spreading-on-the-right-may-hamper-vaccine-efforts-152843610.html
But here is a surprise, the poll found that 15 percent of MSNBC viewers also believe this conspiracy theory. They chose to target Gates specifically because of his decade-long advocacy for vaccines.
So, just for fun, I decided to trace this narrative back to its source. And guess what: I found it. As Reuters Fact Check reported:
“This claim was originally posted as satire on May 13, 2020. Its author, Sam Powell ( here ) later described the post on his Facebook profile as “a wild exaggeration of false rumors already circulating” about Bill Gates and microchips.
“I stretched it to a ridiculous extreme to demonstrate just how willing the right wing extremists are to believe slanderous manipulations of the irrational fears of the anti-vaxxer community to demonize the allegedly liberal Gates and support their false tin idol Trump”, Powell wrote on Facebook, describing the post as a “subtle parody” ( here ).
He is a tad more demonizing of the right than I would like, but it doesn’t change the facts behind what happened next. The parody gained legitimacy and exploded when Fox primetime host Laura Ingraham shared a tweet where she expressed agreement with a user who wrote about the debunked conspiracy theory. She wrote, “Digitally tracking Americans’ every move has been a dream of the globalists for years. This health crisis is the perfect vehicle for them to push this.”
Thanks to Ingraham’s endorsement, different iterations of the claim have now been shared thousands and thousands and thousands of times. Examples of the post are visible here and here.
So, there ya go! I realize the information will not change any of the minds of those who are now emotionally invested in the theory. But at least you now know that it started as parody and how it gained legitimacy. So, there is that.
There Is an Important Number that No One Is Talking About

All the talking heads and politicians talk about testing, the number of people who get COVID-19, and the number who die. Or as the President likes to say, “99 percent of virus cases are harmless.”
But that’s not true. There’s an extremely important missing number here.
First of all, to be precise, the official mortality rate in the U.S. is not 1% as the President claims. It is 3.4%. But that’s because we don’t test enough. As I mentioned earlier, the mortality rate would go down with adequate testing. In fact, when all is said and done, the real mortality rate for COVID-19 is probably as low as 0.6%–especially now as more therapeutics like remdesivir come into play. But that does not mean the President is correct.
When it comes to COVID-19, we cannot limit our discussion to living and dying. This virus has significant morbidity even for those who do not die. About 40 percent of adults in the U.S. have at least one underlying health condition that would put them at risk for severe complications of COVID-19, according to a report published by the Centers for Disease Control and Prevention.5 Hilda Razzaghi, Yan Wang, Hua Lu, et al. “Estimated County-Level Prevalence of Selected Underlying Medical Conditions Associated with Increased Risk for Severe COVID-19 Illness — United States, 2018.” CDC MMWR. July 24, 2020 / 69(29);945–950. (Accessed 4 Aug 2020.) https://www.cdc.gov/mmwr/volumes/69/wr/mm6929a1.htm The bottom line is that some 20% of those who come down with COVID, although they survive, find that the virus is anything but harmless. Many people, even young people, get extremely ill, and their road back to health includes weakness, shortness of breath, loss of muscle mass, and sometimes strokes. As we have discussed previously, COVID-19 can cause brain inflammation, hallucinations, psychosis, delirium, and nightmares. It can scar the lungs horribly, lead to weight loss and loss of lean muscle mass and has even been responsible for strokes in those age 40 and younger and loss of legs due to blood clotting issues. This virus not only affects the lungs and blood, but also the kidneys, liver, and brain–the last potentially resulting in chronic fatigue and major long-term depression, among other symptoms. It may not kill a high percentage, but it does still ravage a significant percentage of people.
A Dutch report published in early July (an excerpt is translated here) surveyed 1,622 Covid-19 patients with an average age of 53 who reported a number of enduring symptoms, including intense fatigue (88%), persistent shortness of breath (75%), and chest pressure (45%). Ninety-one percent of the patients were not hospitalized, suggesting they suffered these side-effects despite their cases of COVID-19 qualifying as “mild”. While 85% of the surveyed patients considered themselves generally healthy before having COVID-19, only 6% thought so one month or more after getting the virus.
Conservatively, you are looking at 10 times the number of people who die from COVID-19 having long-term health issues. When you add in those who suffer long-term harm from the virus, we’re not talking 160,000. We’re talking several million people. So no, it is not “harmless” for 99%.
Children and Schools

There is a passionate, raging debate right now when it comes to opening schools. There are parents and teachers on both sides of the question. Some of it is political, but I’m not going to go into that side of it. I just want to talk about the safety aspect.
On the open now side, there are two main points.
- There is some evidence that children are less likely to catch the virus versus adults, and when they do, they are less likely to get as sick.6 Jim Morrison. “What Scientists Know About How Children Spread COVID-19.” Smithsonian Magazine. July 23, 2020. (Accessed 30 Jul 2020.) https://www.smithsonianmag.com/science-nature/what-scientists-know-about-how-children-spread-covid-19-180975396/ Although the evidence leans in that direction, it is ambiguous at best, and even if true, it only applies to children under 10. At 10 and up, their susceptibility is the same as any adult’s. But even for younger children, “less likely” does not mean “not at all.”
- There is also evidence to suggest that children are also less likely to transmit the virus VS adults.7 Morrison Again, the evidence is highly ambiguous–and again, if true, only for children under 10. At 10 and up, their communicability is the same as any adult’s. And again, even for younger children “less likely” does not mean “not at all.”
On the stay closed side, there are the facts on the ground.
- Two weeks after Israel fully reopened schools, a COVID-19 outbreak swept through classrooms — including at least 130 cases at a single school.8 Daniel Estrin. “After Reopening Schools, Israel Orders Them To Shut If COVID-19 Cases Are Discovered.” NPR. June 3, 2020. (Accessed 30 Jul 2020.) https://www.npr.org/sections/coronavirus-live-updates/2020/06/03/868507524/israel-orders-schools-to-close-when-covid-19-cases-are-discovered , 9 TOI Staff. “Almost 10,000 students, teachers quarantined as 217 infected in Israeli schools.” The Times of Israel. 2 Jun 2020. (Accessed 30 Jul 2020.) https://www.timesofisrael.com/thousands-more-students-quarantined-as-nationwide-school-infections-continue/
- A summer camp in suburban Dallas was forced to close less than two weeks after opening when both children and counselors showed symptoms and tested positive for COVID-19.10 Meredith Yeomans. “Summer Camps Struggle to Keep Out COVID-19.” 5 NBCDFW. July 8, 2020. (Accessed 30 Jul 2020.) https://www.nbcdfw.com/news/coronavirus/summer-camps-struggle-to-keep-out-covid-19/2403236/ The camp had put numerous safety precautions in place, including mask wearing, daily temperature checks, social distancing of age groups, no food or material sharing, and much more. Similar outcomes were seen in Oklahoma and Missouri where dozens caught the virus.
- Several weeks ago, 260 of the 597 children attending a summer camp in Georgia contracted the coronavirus, adding to a growing body of evidence that minors are both susceptible to infection and serve as vectors of transmission. According to the CDC, the true number of infected campers was probably significantly higher since test results were only available for 58 percent of the group.
- As of June 30th, there were 950 reported positive cases of COVID-19 in Texas at 668 childcare locations–307 children and 643 staff members.11 Reese Oxner. “More than 300 children in Texas day cares have caught COVID-19, and the numbers are rising.” The Texas Tribune. July 1, 2020. (Accessed 30 Jul 2020.) https://www.texastribune.org/2020/07/01/texas-day-care-coronavirus-cases-rising/ Statewide, 12,207 licensed childcare operations were open at the time, and total reported coronavirus cases had risen from 59 cases in mid-May and 576 on June 23.
- One of the first school districts in the country to reopen its doors during the coronavirus pandemic did not even make it a day before a call from the county health department notified Greenfield Central Junior High School in Indiana that a student who had walked the halls and sat in various classrooms had tested positive for the coronavirus. “We knew it was a when, not if,” said Harold E. Olin, superintendent of the Greenfield-Central Community School Corp., but were “very shocked it was on Day 1.”
- And finally, a study published online in JAMA Network found that infected children have at least as much of the coronavirus in their noses and throats as infected adults, according to the research. Indeed, children younger than age 5 may host up to 100 times as much of the virus in the upper respiratory tract as adults.12 Heald-Sargent T, Muller WJ, Zheng X, Rippe J, Patel AB, Kociolek LK. “Age-Related Differences in Nasopharyngeal Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Levels in Patients With Mild to Moderate Coronavirus Disease 2019 (COVID-19).” JAMA Pediatr. Published online July 30, 2020. https://jamanetwork.com/journals/jamapediatrics/fullarticle/2768952
And then there are the teachers.
- Thirty percent of elementary school teachers are age 50 or older, which puts them in a high-risk group.
- In mid-July, a longtime Arizona elementary school teacher died of coronavirus after sharing a summer classroom with two other teachers who also fell ill with the disease.13 Elisha Fieldstadt. “Beloved Arizona teacher dies of coronavirus, two others sharing classroom also infected.” NBC News. July 13, 2020. (Accessed 30 Jul 2020.) https://www.nbcnews.com/news/us-news/beloved-arizona-teacher-dies-coronavirus-two-others-sharing-classroom-also-n1233672 They were teaching virtual summer school lessons, and the educators “took extra precautions” and “followed the CDC guidelines and more,” but still got sick. They kept their distance, wore masks, and constantly used hand sanitizer.14 James Doubek. “A Teacher Who Contracted COVID-19 Cautions Against In-Person Schooling.” NPR. July 14, 2020. (Accessed 30 Jul 2020.) https://www.npr.org/sections/coronavirus-live-updates/2020/07/14/890716897/teacher-recovering-from-covid-19-says-school-reopening-is-tough-decision
- At least 600 Florida teachers have requested living wills as they prepare for schools in the state to reopen even as coronavirus numbers swell.15 J. Edward Moreno. “Hundreds of Florida teachers request living wills as they prepare to return to school amid COVID-19 spike.” The Hill. 07/25/20. (Accessed 30 Jul 2020.) https://thehill.com/homenews/state-watch/509026-hundreds-of-florida-teachers-request-living-wills-as-they-prepare-to
So, let’s cut to the chase. The primary argument I hear in favor of opening schools is that other countries all over the world are safely opening schools (not counting Israel and France,16 Daniel Cole/AP. “70 cases of COVID-19 at French schools days after reopening.” NBC News. May 18, 2020. (Accessed 30 Jul 2020.) https://www.nbcnews.com/health/health-news/70-cases-covid-19-french-schools-days-after-re-opening-n1209591 of course), so why shouldn’t the United States?
And the simple answer is lava!
When lava is hot and fresh and flowing, it’s not a good idea to walk on it. Once it has cooled, though, there is no problem walking on it. In fact, if you wait long enough, after the lava breaks down into volcanic soil, the lava field is not just safe to walk on, it is absolutely verdant.


So, the simple answer as to why other countries can safely open schools and we cannot in the many, many areas of the country that currently have high infection rates is that they are opening their schools on a cooled lava field, whereas we are trying to open them (at least those in the “hot” districts) on flowing lava fields–metaphorically speaking. (See chart below.)
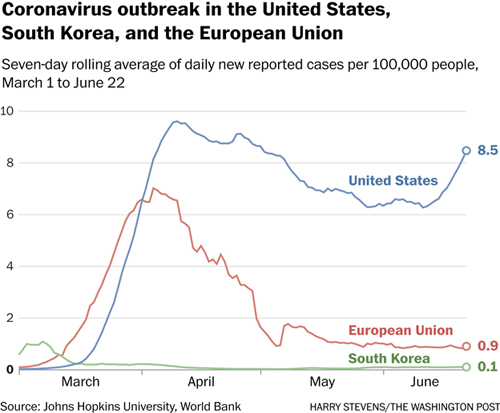
Note: in the above chart, the numbers are not affected by the number of tests. The numbers reflect an average per hundred thousand people. If you test 100,000, 200,000, 1 million people, it doesn’t matter. While the total number of people with the virus would indeed go up, that number never appears in the chart–only the average per 100,000, which would remain unchanged.

Natural Antipathogen Formula as a Prophylactic
One of the things I was challenged on in my last newsletter was that several months earlier I had said there was no need to panic, and now I was preaching doom and gloom and large amounts of dead people. In fact, nothing has changed. I have said from the very beginning that I expected a large number of deaths–and those predictions are proceeding apace. Specifically, what I said is that the coronavirus had a low mortality rate, but that a low rate applied to a large susceptible population (essentially every person living in the United States) would mean a large number of deaths. But what I also said was that there was no need to panic since there are steps you can take that will likely put you on the good side of those numbers. And one of the more essential pieces of that program is an effective natural antipathogen formula.
Since I first mentioned that formula, many people have written in to ask if the natural antipathogen formula could be taken on a daily basis in smaller amounts to prevent ever getting the virus in the first place. The idea would be to use it prophylactically versus waiting until you experience the first symptoms and taking it in larger amounts to throttle back its progression from that point?
That’s an interesting question.
Before we go any further, we need to keep in mind that there is no actual proof that the formula works to kill the virus if you have been infected. Yes, there are thousands of anecdotal testimonials over the years as to how well it works in controlling the flu, but none of this constitutes proof. Without the rigors of a large cohort study, there is no proof that people who didn’t use the formula wouldn’t have had exactly the same experience in terms of either preventing the flu from hitting full on or patients getting well in what appeared to be half the time. And when it comes to the coronavirus, we have far fewer anecdotal reports. There is me, Kristen, and maybe a half dozen others who have written in to say that the formula prevented the virus from progressing. But with the coronavirus, the same might have been claimed by 80% of people who came down with the virus, took nothing to mitigate it, and had no or very mild symptoms.
And if we ever did run a huge cohort study and proved the formula stopped COVID-19 in its tracks, I couldn’t talk about those results. If I did, the formula would be classified as a drug and could only be sold by prescription. And Baseline Nutritionals has no network of pharmaceutical reps to convince doctors to do so. In other words, Baseline would no longer be able to sell the formula.
So, where does that leave us?
For the thousands of people who have used the antipathogen formula over the last two decades, they do not need any studies. Based on their personal experience on multiple occasions, they are convinced the formula works. And their experiences are the reason that months of inventory for that formula was cleaned off the warehouse shelves in a matter of days back in March when people suddenly realized the coronavirus was for real. Which brings us to the question at hand: instead of just using it after you notice symptoms, can you use the antipathogen formula prophylactically to prevent ever getting the virus in the first place?
And the answer is: possibly, yes, theoretically?
Again, although there are many reasons to suspect it might work well for this purpose, there are no studies that prove it does so. In fact, such studies would be almost impossible to conduct. When it comes to assessing protection potential, you are talking about a large cohort study in which you analyze the data from a large cohort of people who were exposed to the virus during the course of the study.
Then you compare the infection and mortality results of those who regularly used the formula with those who did not. Unfortunately, no such cohort exists, nor is there ever likely to be one. So, when it comes to the efficacy of using an antipathogen formula to prevent the virus, you are flying blind. Nevertheless, the formula contains several powerful antivirals, and we do have several decades of testimonials vis-à-vis the flu–so again, it’s theoretically likely. Which brings up the question: if so, how much do you need to take?
We already know that when you are dealing with an all-out infection, you need to take a bottle a day for three to four days until the infection is somewhat under control. After that, 10 droppers a day is sufficient. So, 10 droppers a day is a reasonable starting point. The problem with 10 droppers a day for prophylactic purposes, though, is that you are talking about 5 bottles a month, which would get expensive over several months. My guess, and this is just a guess, is that 5 droppers a day, two days on and one day off should do the trick, or at the very least make it likely that any infection is minimal. At that rate, each bottle would last about 18 days, so you are talking just under two bottles a month–which is a whole lot more economically feasible than five bottles a month.
Also, keep in mind that if you are using the formula that regularly, you will want to be sure to supplement with a good probiotic. Yes, the ingredients in the formula, although antibiotic, are gentle when it comes to your intestinal bacteria. But if you are taking it that regularly for weeks on end, it will begin to negatively impact your intestinal flora. So yes, you will want to supplement with a good probiotic to balance out that effect.
Looking Forward

Unfortunately, thanks to an incoherent response from the highest levels of government, inconsistent messaging from public health officials, the media giving diametrically opposed opinions (depending on what station you listen to), not to mention public antipathy for many of the mitigating recommendations, the fight against COVID-19 in the United States has begun to feel hopeless. As a result, conspiracy theories have replaced science for many, whereas others have simply thrown caution to the wind. Now, instead of working as one country to suppress the virus and emerge slowly and carefully into public life again, people are making up their own rules as they go. And the result is chaos, many more deaths than we should ever have seen, and savage disruption to our economy–not to mention an astonishing number of people who claim the entire thing is a hoax. Without leadership from the top, the national response is fragmenting.
- And if you are waiting for a vaccine, don’t count on it helping very much. If the new vaccines are 50% effective, like the flu vaccine in a good year, and only 50% of the population is willing to take it, we are going to be living with the coronavirus for a number of years to come.
- Some people will be immune because they have already had the virus.
- Some will be immune because they got vaccinated and it worked for them.
- Some will do nothing, take no precautions, refuse to wear masks and social distance, come down with the virus, and count on their doctors to use therapeutics to get them through.
- New therapeutics will help here
- And retail businesses and restaurants will find ways to reopen in the new environment by taking steps to kill the virus in the air and prevent its spread from person to person. For example, there are studies to show that air ionizers can kill airborne viruses.17 Hagbom M, Nordgren J, Nybom R, Hedlund KO, Wigzell H, Svensson L. “Ionizing air affects influenza virus infectivity and prevents airborne-transmission.” Sci Rep. 2015;5:11431. Published 2015 Jun 23. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4477231/. The problem is producing enough negative ions economically to sanitize an entire restaurant or store.18 Plasma Air. “Plasma Air Ionization Proven to Reduce Coronavirus Surrogate MS2 Bacteriophage by 99% in Independent Spanish Testing.” PR NewsWire. Jun 16, 2020. (4 Aug 2020.) https://www.prnewswire.com/news-releases/plasma-air-ionization-proven-to-reduce-coronavirus-surrogate-ms2-bacteriophage-by-99-in-independent-spanish-testing-301076955.html And other studies have shown that far-UVC light can kill airborne coronavirus.19 Buonanno, M., Welch, D., Shuryak, I. et al. “Far-UVC light (222 nm) efficiently and safely inactivates airborne human coronaviruses.” Sci Rep 10, 10285 (2020). https://doi.org/10.1038/s41598-020-67211-2 Bottom line: there are ways to make the air and surfaces in indoor environments anathema to coronavirus transmission–without the need for masks.
- Some will have long-term side effects or die.
- And some will proactively build their immune systems and keep a supply of a good natural antipathogen formula on hand to handle any eventuality.
By default, and without consciously choosing it, the United States appears to be heading for a chaotic, slightly modulated, free fall descent into natural herd immunity. If you think I’m exaggerating, then consider that even as I write this, a quarter of a million bikers from every corner of the country are gathering in South Dakota for nine days for the 80th annual Sturgis Motorcycle Rally. And for those nine days, there will be no social distancing and no wearing of masks. As one of the bikers, Rod Woodruff told the Daily Beast on Wednesday, “We’re just celebrating good old American freedom.”
And they will be bringing whatever they catch in those nine days back to every corner of the country. We are so screwed!
Ultimately, it looks like we’re going to have to live with the virus for a long time. The only question is whether you choose to be proactive, reactive, or hope to hide from it. Some day, it would be nice to return to business as normal.

By the way, it’s probably worth mentioning that the long-term herd immunity thing (options 1-3) may not work out so well in the near-term as the virus is showing a propensity for mutation.20 Kai Kupferschmidt. “The pandemic virus is slowly mutating. But is it getting more dangerous?” Science. Jul. 14, 2020. (Accessed 4 Aug 2020.) https://www.sciencemag.org/news/2020/07/pandemic-virus-slowly-mutating-it-getting-more-dangerous At least one mutation made the virus 10 times more infectious.21 Mark Terry. “Mutated COVID-19 Viral Strain in U.S. and Europe 10 Times More Contagious than Original Strain.” BioSpace Jun 30, 2020. (Accessed 4 Aug 2020.) https://www.biospace.com/article/mutated-covid-19-viral-strain-in-us-and-europe-much-more-contagious/ And a new strain that has just appeared in Vietnam appears to be both more infectious22 TOMOYA ONISHI. “Vietnam fights new COVID-19 strain with higher infection rate.” Nikkei Asian Review. August 3, 2020. (Accessed 4 Aug 2020.) https://asia.nikkei.com/Spotlight/Coronavirus/Vietnam-fights-new-COVID-19-strain-with-higher-infection-rate and more severe. 23 “Alarm in Vietnam after new strain of coronavirus.” 112 UA. 29 July 2020. (4 Aug 2020.) https://112.international/ukraine-top-news/alarm-in-vietnam-after-new-strain-of-coronavirus-53430.html
Note: There is one small positive here. With people working from home and a large number wearing masks and socially distancing (even if not enough to stop COVID-19), it should be enough to drastically reduce the spread of flu this year–ultimately dropping the influenza death toll by more than half.
References
| ↑1 | Kathleen Tuthill. “John Snow and the Broad Street Pump.” UCLA Department of Epidemiology. Nov 2003. (Accessed 20 Jul 2020. https://www.ph.ucla.edu/epi/snow/snowcricketarticle.html) |
|---|---|
| ↑2 | “Global HIV & AIDS statistics–2020 fact sheet.” UNAIDS. (Accessed 20 Jul 2020.) https://www.unaids.org/en/resources/fact-sheet. |
| ↑3 | Margaret Talev. “Axios-Ipsos poll: The skeptics are growing.” AXIOS. Jul 21, 2020. (Accessed 30 Jul 2020.) https://www.axios.com/axios-ipsos-poll-gop-skeptics-growing-deaths-e6ad6be5-c78f-43bb-9230-c39a20c8beb5.html |
| ↑4 | Andrew Romano. “New Yahoo News/YouGov poll shows coronavirus conspiracy theories spreading on the right may hamper vaccine efforts.” Yahoo News. May 22, 2020. (Accessed 31 Jul 2020.) https://news.yahoo.com/new-yahoo-news-you-gov-poll-shows-coronavirus-conspiracy-theories-spreading-on-the-right-may-hamper-vaccine-efforts-152843610.html |
| ↑5 | Hilda Razzaghi, Yan Wang, Hua Lu, et al. “Estimated County-Level Prevalence of Selected Underlying Medical Conditions Associated with Increased Risk for Severe COVID-19 Illness — United States, 2018.” CDC MMWR. July 24, 2020 / 69(29);945–950. (Accessed 4 Aug 2020.) https://www.cdc.gov/mmwr/volumes/69/wr/mm6929a1.htm |
| ↑6 | Jim Morrison. “What Scientists Know About How Children Spread COVID-19.” Smithsonian Magazine. July 23, 2020. (Accessed 30 Jul 2020.) https://www.smithsonianmag.com/science-nature/what-scientists-know-about-how-children-spread-covid-19-180975396/ |
| ↑7 | Morrison |
| ↑8 | Daniel Estrin. “After Reopening Schools, Israel Orders Them To Shut If COVID-19 Cases Are Discovered.” NPR. June 3, 2020. (Accessed 30 Jul 2020.) https://www.npr.org/sections/coronavirus-live-updates/2020/06/03/868507524/israel-orders-schools-to-close-when-covid-19-cases-are-discovered |
| ↑9 | TOI Staff. “Almost 10,000 students, teachers quarantined as 217 infected in Israeli schools.” The Times of Israel. 2 Jun 2020. (Accessed 30 Jul 2020.) https://www.timesofisrael.com/thousands-more-students-quarantined-as-nationwide-school-infections-continue/ |
| ↑10 | Meredith Yeomans. “Summer Camps Struggle to Keep Out COVID-19.” 5 NBCDFW. July 8, 2020. (Accessed 30 Jul 2020.) https://www.nbcdfw.com/news/coronavirus/summer-camps-struggle-to-keep-out-covid-19/2403236/ |
| ↑11 | Reese Oxner. “More than 300 children in Texas day cares have caught COVID-19, and the numbers are rising.” The Texas Tribune. July 1, 2020. (Accessed 30 Jul 2020.) https://www.texastribune.org/2020/07/01/texas-day-care-coronavirus-cases-rising/ |
| ↑12 | Heald-Sargent T, Muller WJ, Zheng X, Rippe J, Patel AB, Kociolek LK. “Age-Related Differences in Nasopharyngeal Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Levels in Patients With Mild to Moderate Coronavirus Disease 2019 (COVID-19).” JAMA Pediatr. Published online July 30, 2020. https://jamanetwork.com/journals/jamapediatrics/fullarticle/2768952 |
| ↑13 | Elisha Fieldstadt. “Beloved Arizona teacher dies of coronavirus, two others sharing classroom also infected.” NBC News. July 13, 2020. (Accessed 30 Jul 2020.) https://www.nbcnews.com/news/us-news/beloved-arizona-teacher-dies-coronavirus-two-others-sharing-classroom-also-n1233672 |
| ↑14 | James Doubek. “A Teacher Who Contracted COVID-19 Cautions Against In-Person Schooling.” NPR. July 14, 2020. (Accessed 30 Jul 2020.) https://www.npr.org/sections/coronavirus-live-updates/2020/07/14/890716897/teacher-recovering-from-covid-19-says-school-reopening-is-tough-decision |
| ↑15 | J. Edward Moreno. “Hundreds of Florida teachers request living wills as they prepare to return to school amid COVID-19 spike.” The Hill. 07/25/20. (Accessed 30 Jul 2020.) https://thehill.com/homenews/state-watch/509026-hundreds-of-florida-teachers-request-living-wills-as-they-prepare-to |
| ↑16 | Daniel Cole/AP. “70 cases of COVID-19 at French schools days after reopening.” NBC News. May 18, 2020. (Accessed 30 Jul 2020.) https://www.nbcnews.com/health/health-news/70-cases-covid-19-french-schools-days-after-re-opening-n1209591 |
| ↑17 | Hagbom M, Nordgren J, Nybom R, Hedlund KO, Wigzell H, Svensson L. “Ionizing air affects influenza virus infectivity and prevents airborne-transmission.” Sci Rep. 2015;5:11431. Published 2015 Jun 23. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4477231/. |
| ↑18 | Plasma Air. “Plasma Air Ionization Proven to Reduce Coronavirus Surrogate MS2 Bacteriophage by 99% in Independent Spanish Testing.” PR NewsWire. Jun 16, 2020. (4 Aug 2020.) https://www.prnewswire.com/news-releases/plasma-air-ionization-proven-to-reduce-coronavirus-surrogate-ms2-bacteriophage-by-99-in-independent-spanish-testing-301076955.html |
| ↑19 | Buonanno, M., Welch, D., Shuryak, I. et al. “Far-UVC light (222 nm) efficiently and safely inactivates airborne human coronaviruses.” Sci Rep 10, 10285 (2020). https://doi.org/10.1038/s41598-020-67211-2 |
| ↑20 | Kai Kupferschmidt. “The pandemic virus is slowly mutating. But is it getting more dangerous?” Science. Jul. 14, 2020. (Accessed 4 Aug 2020.) https://www.sciencemag.org/news/2020/07/pandemic-virus-slowly-mutating-it-getting-more-dangerous |
| ↑21 | Mark Terry. “Mutated COVID-19 Viral Strain in U.S. and Europe 10 Times More Contagious than Original Strain.” BioSpace Jun 30, 2020. (Accessed 4 Aug 2020.) https://www.biospace.com/article/mutated-covid-19-viral-strain-in-us-and-europe-much-more-contagious/ |
| ↑22 | TOMOYA ONISHI. “Vietnam fights new COVID-19 strain with higher infection rate.” Nikkei Asian Review. August 3, 2020. (Accessed 4 Aug 2020.) https://asia.nikkei.com/Spotlight/Coronavirus/Vietnam-fights-new-COVID-19-strain-with-higher-infection-rate |
| ↑23 | “Alarm in Vietnam after new strain of coronavirus.” 112 UA. 29 July 2020. (4 Aug 2020.) https://112.international/ukraine-top-news/alarm-in-vietnam-after-new-strain-of-coronavirus-53430.html |







