
In this newsletter, we turn to the large intestine, or colon, which absorbs any remaining water in the feces and transfers them to the rectum for excretion. We also explore all of those things that can go wrong in the colon and the options you have for correcting them.
 Written By: Jon Barron
Written By: Jon Barron
And now we are ready to conclude our series on the intestinal tract. Several months ago, we began at the top of the tract, in the mouth. We followed our meal step-by-step as it moved on down the esophagus into the stomach where initial digestion began. We then moved into the duodenum and the small intestine where digestion was completed and absorption took place. Now, in this newsletter, we turn to the large intestine, or colon, which absorbs any remaining water in the feces and transfers them to the rectum for excretion. As part of our exploration, we will also explore the various reflexes that move feces into and through the colon. And finally, we will conclude by examining the complicated anal sphincter muscle that controls passage through the anus and then discussing the physiology of defecation. Along the way, we will also explore those things that can go wrong in the colon — from colon cancer to diverticular disease — and the options you have to correct them.
Let’s begin by looking at the anatomy of the colon, rectum, and anus.
The colon, rectum, and anus
The large intestine (aka the colon or large bowel) is the last part of the digestive system and has two primary functions:
- It extracts water and salt from solid wastes before they are eliminated from the body. It should be noted that by the time chyme enters the large intestine, 90% of its water has already been absorbed in the small intestine. On the other hand, as we saw earlier, absorbing that final ten percent is essential for maintaining proper hydration in the body. If the secretion and absorption of water doesn’t balance, we become either bloated or dehydrated. It’s also essential for firming up the stools and preventing diarrhea. (The large intestine does not play a major role in the absorption of nutrients in the body.)
- It uses bacteria that reside in the colon to ferment and break down any unabsorbed food material that passed through the small intestine unabsorbed. These materials consist largely of amylose (forms of starch), undigested protein, and “indigestible” carbohydrates. The bacteria break down some of these materials for their own nourishment and create acetate, propionate, and butyrate as waste products, which in turn are used by the cell lining of the colon for nourishment. Fermentation by bacteria also produces methane gas, hydrogen gas, and assists in the breakdown of bile salts. Note: intestinal gas is primarily swallowed air. Only 20% consists of the methane and hydrogen produced from fermentation by bacteria.
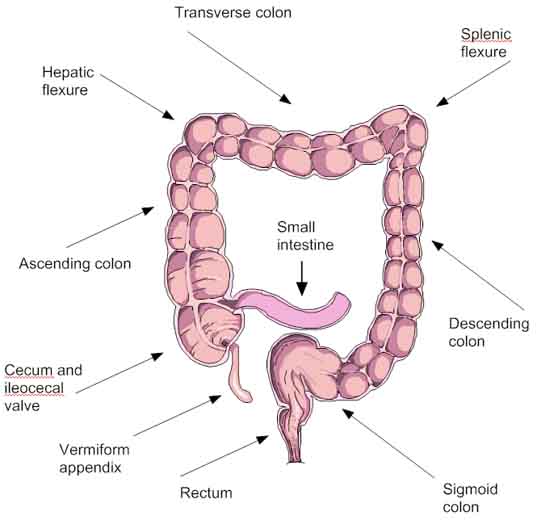
Anatomically, the large intestine begins with an area called the cecum (caecum), which extends on up through the ascending colon, across the body through the transverse colon, then down towards the anus through the descending colon. It ends in an s-shaped “trap” area called the sigmoid colon, which leads to the rectum, and then on out through the anus. In total, it is about five feet (1.5 meters) in length. On average, it is about 2.5 inches wide, but generally starts much wider in the ascending colon and narrows by the time it reaches the sigmoid colon. The pH in the colon varies between 5.5 and 7 (slightly acidic to neutral).
Structurally, the walls of the colon are similar to the small intestine. All of the underlying layers are virtually identical. The serosa (outside covering), muscularis (layer of muscles that control peristalsis), and submucosa (connective tissue), are all the same. The mucosa, the actual surface on the inside of the large intestine, however, is different. Since nutrient absorption is not a factor, there are no villi. Instead, we find a smooth velvety surface with pits dropping deep into the mucosa. The pits are for absorbing water. Note: mucous is secreted by the mucosa to lubricate the colon, but enzymes are not secreted.
The ileocecal valve
The ileocecal valve is actually a fold of muscle controlled mucosa located in the cecum between the small and large intestine that serves as the inlet valve of the colon. It acts as a one way valve to allow food wastes to flow from the small intestines into the first part of the colon, the cecum, but prevents waste in the colon from leaking back into the small intestine. It is the distension of the cecum, caused by the chyme entering from the small intestine that actually triggers the closing of the ileocecal valve. The ileocecal valve also has a second related function — to prevent the contents of the ileum from passing into the cecum prematurely. Note: once chyme (food mixed with digestive juices) passes through the ileocecal valve and enters the cecum, it picks up a new name. It is now designated as fecal matter, and it is still fecal matter if it backs up through a malfunctioning ileocecal valve and reenters the small intestine.
The proper function of the ileocecal valve is to open and close upon demand. When this muscle sticks in the open position, it allows fecal matter back into the small intestine. Not healthy! When the muscle is stuck in the closed position, it causes constipation. The main causes of these two conditions are improper diet and stress; and either condition can seriously affect the body. Alcohol in particular can cause the valve to stick in the open position, resulting in the toxic feeling associated with hangovers.
The cecum
Shaped like a pouch, the cecum (also spelled caecum) is where the colon begins. It sits on the right side of your body (left when viewed from the front as seen from an anatomy POV) and, as already mentioned, is connected to the small intestines through the ileocecal valve. Its sole function is to receive waste from the small intestine as it pours through the ileocecal valve.
Appendix
Located below the ileocecal valve are the vermiform and retrocecal appendixes. The retrocecal appendix is located inside the cecum and rarely causes a problem. The vermiform (“wormlike add-on”) is the familiar appendix that dangles from the cecum and can frequently become inflamed or infected and require surgery. Like the gallbladder, the medical community considers the appendix to be vestigial — an evolutionary holdover primarily used by ruminants for hard to digest foods, particularly woody foods. The thinking is that in people, it’s become less and less important over time — shriveling to a wormlike vestigial organ that gets infected. However, thanks to surgeons who now save anyone with appendicitis, there’s no evolutionary imperative for the appendix to disappear, so it continues. At least that’s the medical thinking.
But as with the gallbladder, that thinking may be a misapprehension, and the vermiform appendix may not be as vestigial as is medically assumed. There is now evidence that the appendix may be of significant importance — that it plays a powerful role in the functioning of the immune system and that it serves as a storage area for beneficial bacteria.
According to a paper published in the Journal of Evolutionary Biology, the appendix serves a dual function. First, it makes, trains, and directs white blood cells. Second, it serves as a type of warehouse or storage compartment for “good bacteria” that boost the immune system when help is required. According to the research, the appendix holds on to reserves of “good bacteria” so that when bad bacteria flourish or a nasty case of diarrhea reduces the colonies of good bacteria, the appendix can send in reinforcements. These bacteria may also influence white blood cells to clear up any infections in the gut. The studies cited in the paper clearly indicate that the appendix does indeed influence white cell function. So once again, it appears medical science may have “vestigialized” an important functioning organ.
The traffic junction
The three organs just discussed, the cecum, the ileocecal valve, and the appendix form what can be described as a traffic junction designed to control the flow of waste into the large intestine. Ideally, they should be cleared of waste on a continual basis — daily at the very least.
This can most easily be achieved by using the squatting position when evacuating your bowels. (If you are not presently visiting a rural village in India where the toilet is a hole in the ground, you can always use a toilet footstool.)
As Jonathan Isbit explains on his website, Nature’s Platform,1 Jonathan Isbit. Natures Platform. http://www.naturesplatform.com in the squatting position, the left thigh supports the descending and sigmoid colons so as to minimize straining and help squeeze fecal matter on into the rectum for imminent evacuation. In addition, the squatting position helps relax the rectal muscles to facilitate evacuation. Meanwhile, the right thigh presses against the lower abdomen on the right side of the body, thereby “squeezing” the cecum to force waste upwards into the ascending colon and away from the appendix, ileocecal valve, and small intestines.
As a result of waste being pushed up out of the cecum, the appendix is kept free of waste and is unlikely to ever get infected. In addition, pressure from the right thigh also helps the ileocecal valve stay securely closed to guard against any leakage of waste into the small intestine. Finally, as the result of the reduced pressure required for evacuation, the squatting position is a highly effective treatment/preventative for hemorrhoids.
The large intestine
Once fecal matter arrives in the cecum, it begins its journey through the rest of the large intestine and on out of the body. The ascending colon, on the right side of the abdomen, is about 25 cm (10 inches) long in humans. It extends from the cecum straight up the right side of your abdominal cavity to just under the liver, where it makes a sharp right angle bend to the left (in what is known as the hepatic flexure) and becomes the transverse colon. The ascending colon receives fecal material as a liquid. The muscles of the colon then move the watery waste material forward and slowly begin the absorption of all excess water.
The transverse colon runs straight across the body from right to left, from the hepatic flexure to what is called the splenic flexure (the right angle bend on the left side of the body just below the spleen). As you may remember from our last newsletter, the transverse colon hangs off the stomach, attached to it by the greater omentum. It is about 18 inches long.
The transverse colon is unique among the other parts of the large intestine in one important way: it is mobile. The ascending, descending, and sigmoid colons are pretty much locked into place and do not move noticeably. Not so for the transverse colon. This becomes particularly important later in the newsletter when we talk about prolapsed colons. It should also be noted that colon cancer starts to become more frequent as we enter the transverse colon, with its incidence steadily increasing as we move further along the bowel, peaking when we reach the sigmoid colon and the rectum. One other note on the transverse colon: in some people who are not evacuating their bowels properly, it can become a major storage area for fecal matter. Again, this will be a factor when we talk about prolapsed colons.
The descending colon runs from the end of the transverse colon on the left side of the body, from the splenic flexure to the beginning of the sigmoid colon and is about 12 inches in length. The function of the descending colon in the digestive system is to store food that will be emptied into the rectum. It is also in the descending colon that stools start to become semi solid as they move on to the sigmoid colon.
The sigmoid colon is about 18 inches long and is S-shaped. In fact, sigmoid means S-shaped. It begins just after the descending colon and ends just before the rectum. Stools more or less complete their solidification in the sigmoid colon. Additionally, the walls of the sigmoid colon are muscular and contract to forcefully “move” stools into the rectum.
The rectum begins at the end of the sigmoid colon and is about four to six inches in length. It is defined by its powerful muscles and by the fact that it sits outside the peritoneal lining (the lining of the abdominal cavity). Essentially, the rectum serves as a holding area for fecal matter. Internally, the rectum contains little transverse folds that serve to keep the stool in place until you’re ready to go to the bathroom. When you’re ready, the stool enters the lower rectum, moves into the anal canal, and then passes through the anus on its way out. Stimulus of the rectum (giving you the urge to go to the bathroom) occurs both internally (which is an involuntary stimulus) and externally (which occurs when you voluntarily squeeze the muscles. Note: by the time they reach the rectum, feces are composed of water salts, desquamated (peeled off or shed) epithelial cells, bacterial decay products, and undigested food (fiber, etc.). Also, the rectum is an excellent absorber. It can be used to instill (insufflate) water, salts, medication, and/or herbs rapidly — almost as fast as if administered intravenously.
The anus is the end of the trail. Its function is to control the expulsion of feces. The flow of fecal matter through the anus is controlled by the anal sphincter muscle.
Physiology of defecation
 The feces end up in the rectum via mass peristalsis. Receptors signal distension of the rectum to the brain. This is a conscious perception. The defecation reflex is initiated when parasympathetic (involuntary) stimulation from the spinal cord contracts the longitudinal rectal muscles. This causes pressure to increase in the rectum. Pressure is added to the rectum by voluntary contraction of the abdominal muscles. Parasympathetic stimulation (again involuntary) relaxes the internal sphincter of the anus. This increases the urge to defecate. Finally, the external sphincter is opened by voluntary relaxation, which allows the feces to pass out of the body. This can be postponed by voluntary contraction. This is useful since it allows us to wait for an appropriate time/place to go to the bathroom. However, continually postponing defecation begins to dull the evacuation response over time — leading to chronic constipation. Then again, voluntary postponement can be overwhelmed by conditions such as diarrhea or long term weakening of the muscles. And finally, sphincter muscles weakened by age, disease, or trauma can cause incontinence (inability to hold feces in). Note: bulky, indigestible fiber acts like a “colonic broom” to move feces through the system more quickly, carrying fat, cholesterol, and carcinogens with it.
The feces end up in the rectum via mass peristalsis. Receptors signal distension of the rectum to the brain. This is a conscious perception. The defecation reflex is initiated when parasympathetic (involuntary) stimulation from the spinal cord contracts the longitudinal rectal muscles. This causes pressure to increase in the rectum. Pressure is added to the rectum by voluntary contraction of the abdominal muscles. Parasympathetic stimulation (again involuntary) relaxes the internal sphincter of the anus. This increases the urge to defecate. Finally, the external sphincter is opened by voluntary relaxation, which allows the feces to pass out of the body. This can be postponed by voluntary contraction. This is useful since it allows us to wait for an appropriate time/place to go to the bathroom. However, continually postponing defecation begins to dull the evacuation response over time — leading to chronic constipation. Then again, voluntary postponement can be overwhelmed by conditions such as diarrhea or long term weakening of the muscles. And finally, sphincter muscles weakened by age, disease, or trauma can cause incontinence (inability to hold feces in). Note: bulky, indigestible fiber acts like a “colonic broom” to move feces through the system more quickly, carrying fat, cholesterol, and carcinogens with it.
Things that can go wrong
According to medical doctors, digestion time (from entering your mouth to passing through your anus) varies depending on the individual. For healthy adults, according to the Mayo Clinic, “It’s usually between 24 and 72 hours. After you eat, it takes about six to eight hours for food to pass through your stomach and small intestine. Food then enters your large intestine (colon) for further digestion and absorption of water. Elimination of undigested food residue through the large intestine usually begins after 24 hours. Complete elimination from the body may take several days.” That means that, medically speaking, constipation is defined as anything fewer than three bowel movements per week. Or conversely, that normal could be defined as slightly less than one bowel movement every other day.
Quite simply, that’s nonsense. It’s merely the average elimination time that most doctors see in their patients. But keep in mind, 99% of those patients are eating the standard, fast food, highly processed, low fiber, modern diet. That’s neither healthy nor “normal.” It’s merely what most people do, and most people are unhealthy — or rapidly moving in that direction. In fact, normal digestion/elimination time is about 24 hours. You literally should have one major bowel movement for every meal you had the day before. You should be passing the waste from yesterday’s breakfast when you get up in the morning, or shortly after today’s breakfast. Yesterday’s lunch should pass around lunchtime and dinner around dinner time. Holding waste in the colon for longer periods of time is one of the single biggest factors in the onset on many major diseases — not just the colon specific diseases we will discuss below.
Colon cleansing
Other than eating a healthy, high fiber, largely raw food diet, the single best thing you can do for your overall health and the health of your colon is a semi-annual colon cleanse. Any program designed to improve our health or to eliminate disease from our bodies must begin with intestinal cleansing and detoxification. It is the “sine qua non” of health (literally, “without which, there is not”).
Look for a program that addresses all of the following aspects of intestinal health:
 Remove all old fecal matter and waste from the colon (to clear the drain, if you will).
Remove all old fecal matter and waste from the colon (to clear the drain, if you will).- Help remove all the heavy metals and drug residues that have accumulated in the body as a result of having your drain plugged.
- Strengthen the colon muscle so that it works again.
- Repair any damage, such as herniations and inflammations of the colon and small intestine.
- Eliminate the presence of polyps and other abnormal growths that have been allowed to flourish because of an unhealthy intestinal environment.
- Rebuild and replenish the various “friendly” bacteria cultures that ideally should line virtually every square inch of the tube — again, from mouth to anus.
Surgical terminology
A minor digression before we continue! It probably would make sense to define a handful of surgical terms that you are likely to hear from your doctor if you ever have to visit her for any of the conditions below.
- ‘tome — to cut
- ‘ectomy — to cut out, as in appendectomy and cholecystectomy
- ‘otomy — to cut open and then close again, as in colotomy
- ‘ostomy — to cut open and make (semi) permanent, as in colostomy
Colon cancer
The most obvious place we see problems associated with not regularly evacuating the bowels is when it comes to colon cancer. Feces remain in the colon for a long time, and carcinogens in feces (which are concentrated to their maximum degree at that point) are currently assumed to explain the prevalence of colon cancer — second only to lung cancer in the number of deaths it causes each year in the US.
 Fecal matter maintains contact with the wall of the large intestine wall for many hours (sometimes for many days if not effectively clearing your bowels on a daily basis). The longer the contact, the greater the problem. The more severe the constipation, the greater the problem. If this fecal matter contains carcinogens ingested with the diet, those carcinogens (some of which are found in grilled meat) have an excellent chance of affecting the wall of the colon — particularly at places of the longest contact. Not surprisingly, the longest contact and the highest incidence of colon cancer occur in the sigmoid colon, just above the rectum and in the rectum itself.
Fecal matter maintains contact with the wall of the large intestine wall for many hours (sometimes for many days if not effectively clearing your bowels on a daily basis). The longer the contact, the greater the problem. The more severe the constipation, the greater the problem. If this fecal matter contains carcinogens ingested with the diet, those carcinogens (some of which are found in grilled meat) have an excellent chance of affecting the wall of the colon — particularly at places of the longest contact. Not surprisingly, the longest contact and the highest incidence of colon cancer occur in the sigmoid colon, just above the rectum and in the rectum itself.
Societies that eat high fiber, unprocessed diets (that move through the colon more quickly) have far lower incidences of colon cancer, diverticulitis, appendicitis, and coronary artery disease. That said, high fiber diets and proper elimination are not the only factors involved in colon cancer. You can still get colorectal cancer even if you do everything right. Genetics may play a role in up to 10% of colon cancers, for example. Exposure to toxins may also play a factor. Rancid fats in the diet (vegetarian included), too many Omega-6 fatty acids as found in most vegetable oils, and of course, a weakened immune system can all contribute to a higher risk of colon cancer. As always with issues of health, it’s a question of odds…not guarantees.
Polyps
 A polyp is a projecting mass of overgrown tissue. It looks a lot like an inflated balloon, with the part you tie off attached to wherever it’s growing from. Although it is not cancerous itself, virtually all colorectal cancer develops from polyps. When identified during a colonoscopy, polyps are snipped out on the spot thereby eliminating the risk of cancer…from that particular polyp. The same things that cause colon cancer are the things that cause polyps.
A polyp is a projecting mass of overgrown tissue. It looks a lot like an inflated balloon, with the part you tie off attached to wherever it’s growing from. Although it is not cancerous itself, virtually all colorectal cancer develops from polyps. When identified during a colonoscopy, polyps are snipped out on the spot thereby eliminating the risk of cancer…from that particular polyp. The same things that cause colon cancer are the things that cause polyps.
Prolapsed colon (Ptosis)
Ptosis is defined as the abnormal descent (prolapse) of the transverse colon in the abdominal cavity. It is usually associated with the downward displacement of other viscera. It is actually quite common, although the degree to which the transverse colon may prolapse can vary wildly — from very mild to a full V shape, with the middle of the colon actually dropping down all the way to the pelvis. It also should be noted that it is rare for the transverse colon to prolapse by itself without being accompanied by the prolapse of other abdominal organs. In fact, the term now most commonly used to refer to the condition is enteroptosis (entero referring to the entire intestinal area), which reflects this multi-organ reality. The condition will place pressure on all of the organs under it — uterus, ovaries, prostate, gonads, and bladder. It will exacerbate any tendency towards constipation and will decrease circulation to all of the organs in the lower half of the abdominal cavity. Also, the more pronounced the condition is, the more likely it is to produce a lower “belly bulge” that won’t go away no matter how much weight you lose or scrawny the rest of your body becomes.
The condition is more common in women than men and, in fact, frequent pregnancy is sometimes hypothesized as a contributing factor. But the truth is that although many causes (congenital anomalies, weakness of abdominal muscles from lack of exercise, heavy lifting, etc.) are all suspected, no definitive cause has been found. But there can be no doubt that storing undefecated fecal matter in the transverse colon while awaiting the slow evacuation of the bowels cannot help. In some people, pounds of old fecal matter can be found in the transverse colon waiting a chance to exit the body. And considering that constipation is far more common in women than in men, this would also account for the prevalence of ptosis in women.
How do you treat a prolapsed colon? Actually, medical science has little to offer in the way of help. Surgery is problematic and only rarely helpful. Instead, you need to rebuild your intestinal foundation so as to once again fully support the transverse colon. It is difficult to “fully” reverse a prolapsed colon once it has occurred, but it is possible to “mostly” reverse it — at least to the point it is no longer visible and no longer noticeably impacts your overall health. Protocol includes:
- An intestinal cleanse to remove any accumulated fecal matter in the transverse colon, thereby decreasing the weight of the organ, and therefore its tendency to prolapse.
- Use a toilet footstool to get your feet up to a squatting position to optimize your posture for more effective evacuation.
- Start exercising your abdominal muscles — all of them. This means not just things like sits up, but more yoga based exercises such as uddiyana bhanda that actually lift the internal organs.
- Incorporate inverted postures such as a yoga shoulder stand or an inversion machine to hang upside down and let gravity do the work. Or just use a slant board to get your feet and lower body higher than your head.
- Walk.
- And deep massage that incorporates intestinal work can also help.
Crohn’s, IBS, Ulcerative Colitis
More Americans are hospitalized for digestive diseases than for any other type of illness. In fact, digestive diseases cost the United States alone an estimated $91 billion annually in health care costs, lost work days and premature deaths. And the bottom line is that virtually every single American will suffer from some form of chronic digestive disorder if they live long enough — and the rest of the world is following close behind.
Four years ago, I wrote a newsletter on Crohn’s disease, IBS, and ulcerative colitis. The information and recommendations still apply today.
Diverticular disease
Diverticular disease represents one of the great conflicts between the alternative health community and the medical community. For several decades from the early 1900’s to the 1940’s, the alternative health community vehemently argued that the “modern” diet was creating outpouchings or herniations of the colon. The medical community’s equally vehement response was that this was utter nonsense. After all, they argued, “We perform numerous autopsies and never see any evidence of it.” And they called alternative health practitioners quacks. Nevertheless, starting in the 50’s, they began to take possession of the problem and named it diverticulosis. And as is typical, they gave no acknowledgement to the members of the alternative health community such as John Harvey Kellogg, M.D., who identified the disease almost a half century before they did. Nor was there any acknowledgement that they had missed identifying the condition throughout almost a half century of autopsies — something worth keeping in mind the next time you hear the medical community say that today’s autopsies never provide any evidence of people retaining large amounts of old fecal matter in their colons.
Bragging rights aside, it is now understood by all concerned that many people have small pouches in the lining of their colon that bulge outward through weak spots. Each pouch is called a diverticulum. Multiple pouches are called diverticula. The condition of having diverticula is called diverticulosis. About 10 percent of Americans older than 40 have diverticulosis. About half of all people older than 60 have diverticulosis. The incidence of diverticulosis has increased dramatically from just 10 percent of the adult population over the age of 45 who had this disease in 1952 to an astounding “every person will have many” diverticula, if they live long enough, according to the 1992 edition of the Merck Manual. We’ve certainly come a long way since the medical community’s denial of the first half century.
Comparison of digestive tract length
Back in September when we started this series on the digestive tract, I announced that as we proceeded, we would be comparing the digestive systems of humans to other animals to see what conclusions could be drawn as to what diet we should eat. And we have done that. We’ve compared teeth and seen that human teeth are nothing like the teeth of carnivores. We’ve compared stomachs and seen that once again, the human stomach is very different from that of carnivores and omnivores. In fact, when it comes to teeth and stomachs, humans most closely resemble animals that eat a diet that is mostly comprised of fresh fruit, vegetables, and nuts — with, in some instances, a bit of raw meat thrown in for good measure.
Is this important?
Yes! The medical community bases its assumptions concerning the human digestive system on the “fact” that it is essentially designed as an omnivore system. But as I discussed in detail in Lessons from the Miracle Doctors (and so far in this series on the digestive tract), this is simply not supported by the evidence at hand. This distinction is not subtle…and not insignificant. Yes, the human body has an amazing ability to adapt to any diet we throw at it — but not without consequences. And, in fact, many of the diseases we face today are the direct result of not understanding what our systems are designed to handle and the consequences we face as a result.
So, in this newsletter, we reach the last point of comparison: the length of the alimentary canal compared to the length of the body.
An examination of the carnivore intestinal tract reveals a short (relative to the length of their body) tract for fast transit of waste out of the body. The actual length of the carnivore bowel (small and large combined) is approximately 3–5 times the length of the body — measured from mouth to anus — a ratio less than half that found in humans. Fast transit of waste for carnivores is essential for two reasons. The faster the transit, the less opportunity for parasites to take hold. Also, meat tends to putrefy in the intestinal tract, so fast transit limits exposure to the byproducts of putrefaction.
As for the herbivore (cows, sheep, etc.) bowel, at 20–28 times the length of the body (from mouth to anus), it usually runs almost eight times longer than a carnivore’s, since plant matter (unlike meat) is not prone to putrefaction, thus rendering quick elimination moot. Again, not much like us.
As for the bowel of the frugivore (gorilla, orangutan, chimpanzee, etc.), it runs about 10–12 times the length of the body from mouth to anus.
So which intestinal tract does the human alimentary canal most closely resemble? As we discussed in our Digestive System Overview, the entire system runs about 30 feet in length from mouth to the anus.
Let’s total up the lengths we’ve identified so far:
- Esophagus equals one foot
- Small intestine equals 23 feet
- Bowel equals five feet (as cited above)
That’s 29 feet. Add in the mouth, stomach, and rectum and you have a total length of approximately 30 feet. Now compare that to the length of the body (mouth to anus). Why mouth to anus and not head to toe? Because when calculating the body length of four legged animals, we don’t stretch out the legs and add them in. We measure from mouth to tail, and so, for a valid comparison, we need to do the same with humans. In any case, mouth to anus is about 2.5 to 3 feet. That gives you a ratio of 10-12 to one. Bingo! It’s an absolute match to the frugivore intestinal tract.
What should we eat?
So, are we restricted to fruits and nuts? No. In fact, the frugivores we most closely resemble, the wild chimpanzees, periodically eat live insects and raw meat. Among the great apes (the gorilla, the orangutan, the bonobo, and the chimpanzee) and ourselves, only humans and chimpanzees hunt and eat meat on a frequent basis. Nevertheless, chimpanzees are largely fruit eaters, and meat comprises only about 3 percent of their diet — far less than is found in the typical Western diet.
Is a vegetarian diet automatically healthier? Not necessarily. Some people actually do better when they include small amounts of meat in their diet — although, to be sure, a balanced vegetarian diet appears to offer some protection against cancer and heart disease. Other factors in our diet, however, affect our health to a much greater degree than whether or not we eat meat. The bottom line is that, ethical questions aside, eating small amounts of meat, chicken, or fish probably comes down mostly to a personal choice. If you choose to, you can include meat in your diet without any significant health problems — with the following provisos:
- Keep the amount small, three ounces a day or less.
- If you’re going to eat meat, eat organic. Eat grass fed beef, free range chicken and eggs, wild caught fish.
- Avoid or minimize dairy. And if you must have it, have it raw — or at the very least free of growth hormones. Remember, heat (pasteurization) denatures proteins, specifically making several dairy proteins relatively indigestible and highly allergenic.
- Include lots of water soluble fiber in your diet to keep the unabsorbed proteins moving through the digestive tract. If nothing else, incorporate a tablespoon of psyllium as part of your daily regimen.
Conclusion
We’ve covered the intestinal tract from mouth to anus over the last five plus months. Specifically, we’ve explored how we get food into the digestive tract, which organs support digestion, how nutrients are absorbed, and how we process and eliminate waste.
So what useful things have we learned?
 It’s important to chew food thoroughly so that it mixes completely with the amylase in your saliva.
It’s important to chew food thoroughly so that it mixes completely with the amylase in your saliva.- Eat raw foods as much as possible so that your food is packed with live enzymes.
- Use digestive enzyme supplements with your meals to compensate for any shortage of live enzymes in your food. Any shortage causes the body to produce excess stomach acid to compensate.
- Do not drink a large amount of fluids (water, soda, beer) with your meals as that dilutes digestive juices, thus forcing the body to produce more excess stomach acid to compensate.
- How to correct excess stomach acid without using antacids or proton pump inhibitors.
- Why antacids ultimately lead to more stomach acid.
- Why proton pump inhibitors ultimately lead to nutrition problems.
- How to use self massage, chiropractic adjustment and special exercises to correct hiatal hernias.
- Why it makes sense to regularly run a liver detox program to clean out your liver, pancreas, gallbladder, and kidneys.
- How to make sure you absorb the vitamins and minerals you eat or supplement with.
- How to rebuild and replenish the various “friendly” bacteria cultures that ideally should line virtually every square inch of the tube — again, from mouth to anus.
- Why it makes sense to regularly run a colon detox program to clean out your intestinal tract — particularly the large intestine.
And that’s it. We’ve covered the anatomy and physiology of everything from your teeth to your bowel, plus the organs of digestion including the liver, gallbladder, and pancreas. And even more importantly, along the way, we’ve explored the nature of diseases of the digestive tract (everything from hiatal hernia to acid reflux, from peptic ulcers to irritable bowel syndrome) and how to treat them naturally by working with your body, not against it.
For those of you who would like to review the previous parts of this series, check out:
- Overview of the Digestive System
- Your Stomach, Part 1
- Your Stomach, Part 2
- Your Stomach, Part 3
- The Pancreas and Digestion
- Understanding the Liver and Cholesterol
- Healing the Liver and Gallbladder
- Anatomy of the Small Intestine
- Physiology of the Small Intestine, Part 1
- Physiology of the Small Intestine, Part 2
References
| ↑1 | Jonathan Isbit. Natures Platform. http://www.naturesplatform.com |
|---|








A lazy colon. Please advise.
A lazy colon. Please advise.
Digests but will not eliminate.
I poop once a week. And sit
I poop once a week. And sit over steam when I want to poop. I bleed when I poop. Please advise me on what to do
Very good article. I was
Very good article. I was having some minor symptoms of polyneuritis, so I did a colonic lavage, 1% NaCl, 2L, temperature about 106 F. Hips elevated, fill descending colon, let it run to the transverse colon, and then turn on my right side, and gently poke cecal region for slight agitation to help slough off adhered materials. I have been eating well, but had a lot of chicken a couple weeks ago and did not fully chew / salivate it. Wow, the lavage was quite successful basis visual observation. 2 hrs. later I feel quite differen and much better. The polyamines and sulfides, di-sulfides, etc. leak into the bloodstream and weaken our oxidation mechanisms. I’ll do some repeats in the upcoming days until they return clear. The above article I found to be very worthwhile, thank you.
The fiber-deficiency theory of diverticular disease was disproved by the Peery study shown here: http://www.ncbi.nlm.nih.gov/pubmed/22062360 . There is no doubt that diverticulosis is caused by the abandonment of squatting in the western world. Footstools will not prevent diverticulosis, because only genuine squatting protects the sigmoid colon adequately.