Under the provisions of the 1990 National Nutrition Monitoring and Related Research Act, every five years, Health and Human Services (HHS) and the US Department of Agriculture (USDA) must jointly publish a report containing nutritional and dietary information and guidelines for the general public. The 2015-2020 edition of the Dietary Guidelines, after due research and public comment, was published in December.1 “Dietary Guidelines for Americans 2015-2020 Eight Edition.” Office of Disease Prevention and Health Promotion, U.S. Department of Health and Human Services. http://health.gov/dietaryguidelines/2015/guidelines/ In today’s newsletter, now that I’ve had a chance to go over it in some detail, we’ll take a look at it.
Goal of the Guidelines
The goal of the report is to assess the current state of scientific knowledge concerning the relationship of diet to health and to make recommendations about the components of a healthy and nutritionally adequate diet that help promote health and prevent chronic disease for current and future generations. Its primary purpose is to “translate science into succinct, food-based guidance that can be relied upon to help Americans choose foods that provide a healthy and enjoyable diet.” Its recommendations are ultimately intended to help people improve and maintain overall health and reduce the risk of chronic disease. Its focus is disease prevention–not disease treatment. Its primary audiences, and this is important, are policymakers as well as nutrition and health professionals, not the general public. This means that even though it affects you profoundly, you probably haven’t heard about it. That said, one key change in this report over previous versions is that it has shifted its emphasis from treating foods in isolation to focusing, rather, on “patterns” of healthy eating and how foods and beverages act synergistically to affect health. This is a change for the better, but, as we will discuss, it still leaves plenty of giant holes in evaluating the effect of diet on health.
In any case–as the report acknowledges, but takes no responsibility for–despite the fact that “essential nutrient” deficiencies have declined dramatically over the last century, the incidence of chronic diet-related diseases has soared. One step forward, one step back. The bottom line is that although packed with synthetic essential vitamins, the modern diet, along with reduced physical activity, has led to significant nutrition- and physical activity-related health challenges. To quote from the Guidelines, “About half of all American adults–117 million individuals–have one or more preventable chronic diseases, many of which are related to poor quality eating patterns and physical inactivity. These include cardiovascular disease, high blood pressure, type 2 diabetes, some cancers, and poor bone health. More than two-thirds of adults and nearly one-third of children and youth are overweight or obese. These high rates of overweight/obesity and chronic disease have persisted for more than two decades and come not only with increased health risks but also at a high cost. In 2008, the medical costs associated with obesity were estimated to be $147 billion. In 2012, the total estimated cost of diagnosed diabetes was $245 billion, including $176 billion in direct medical costs and $69 billion in decreased productivity.”2 “Chronic Disease Prevention and Health Promotion.” CDC. Last updated February 23, 2016. (Accessed 23 Mar 2016.) http://www.cdc.gov/chronicdisease/overview/ Obviously, then, Dietary Guidelines that really worked would be invaluable.
How the Guidelines Are Put Together
HHS and USDA collaborate during a 3-stage process. At first glance the process seems quite reasonable.
- Review the Current Scientific Evidence
- Develop the Dietary Guidelines
- Implement the Dietary Guidelines
But on closer inspection, gaping holes begin to appear.
Stage1: Review of Current Scientific Evidence
In the first stage, the Secretaries of HHS and of USDA appoint an external Dietary Guidelines Advisory Committee. The use of a Federal advisory committee is to ensure that the Federal Government is seeking “sound” external scientific advice to inform policy decisions. Nominations from the public (although you probably were never asked) were sought for candidates to serve on the 2015 Advisory Committee. The 15 members of the Committee are prestigious researchers in the fields of nutrition, health, and medicine. (Note: you don’t actually have to read the following abbreviated bios. Just skim them. They’re presented merely to show you that they’re all part of mainstream medicine and its bastard child, mainstream nutrition. In other words, they are all part of the same establishment and represent the same general viewpoints.)
 Chair: Barbara Millen, Dr.P.H, R.D.: Professor, Department of Family Medicine, Boston University School of Medicine (through 2009). During her 30-year tenure at Boston University, she was the Founding Chairman of the Graduate Programs in Medical Nutrition Sciences, the Associate Dean for Research and Faculty Development of the School of Public Health, the Chairman of the Faculty Council, and Director of Nutrition Research for the internationally-renown Framingham Heart Study.
Chair: Barbara Millen, Dr.P.H, R.D.: Professor, Department of Family Medicine, Boston University School of Medicine (through 2009). During her 30-year tenure at Boston University, she was the Founding Chairman of the Graduate Programs in Medical Nutrition Sciences, the Associate Dean for Research and Faculty Development of the School of Public Health, the Chairman of the Faculty Council, and Director of Nutrition Research for the internationally-renown Framingham Heart Study.- Vice Chair: Alice H. Lichtenstein, D.Sc.: Professor of Nutrition Science and Policy, Friedman School of Nutrition Science and Policy, Tufts University. Dr. Lichtenstein is also Director and Senior Scientist, Cardiovascular Nutrition Laboratory, Jean Mayer USDA Human Nutrition Research Center on Aging.
- Steven Abrams, M.D.: Professor of Pediatrics, Baylor College of Medicine. He is currently a member of the American Academy of Pediatrics Committee on Nutrition and the American Society for Bone and Mineral Research.
- Lucile Adams-Campbell, Ph.D.: Professor of Oncology, Georgetown University Medical Center, Lombardi Comprehensive Cancer Center. She also serves as the Associate Director of Minority Health and Health Disparities Research and Associate Dean of Community Health and Outreach at Georgetown University Medical Center Lombardi Comprehensive Cancer Center.
- Cheryl Anderson, M.P.H., Ph.D.: Associate Professor, Department of Family and Preventive Medicine, School of Medicine, University of California, San Diego. Her research expertise focuses on the influence of dietary sodium and potassium on cardiovascular disease in minority and underserved populations.
- J. Thomas Brenna, Ph.D.: Professor of Human Nutrition, Chemistry and Food Science, Cornell University. He is an expert in the field of fatty acid and lipid metabolism.
- Wayne Campbell, Ph.D.: Professor, Department of Nutrition Science, Purdue University. His expertise includes evaluating the effects of protein, carbohydrate, and energy intakes and exercise training on macronutrient metabolism, body composition, and muscle strength and function.
- Steven Clinton, M.D., Ph.D.: John B. and Jane T. McCoy Chair of Cancer Research, The Ohio State University Comprehensive Cancer Center, and Professor, Division of Medical Oncology, Department of Internal Medicine, The Ohio State University School of Medicine. He has published extensively on the role of dietary energy balance and obesity in cancer risk, on a variety of foods associated with cancer prevention properties, as well as on several nutrients including vitamin D, calcium, omega-3 fatty acids, and vitamin E.
- Gary Foster, Ph.D.: Director, Center for Obesity Research and Education, Laura Carnell Professor of Medicine, Public Health and Psychology, Temple University. He is an international expert on obesity.
- Frank Hu, M.D., Ph.D., M.P.H.: Director, Harvard Transdisciplinary Research in Energetics and Cancer Center, Department of Nutrition, Harvard School of Public Health. He is an expert in the areas of dietary and lifestyle determinants of obesity, type 2 diabetes, and cardiovascular disease.
- Miriam Nelson, Ph.D.: Professor, Friedman School of Nutrition Science and Policy, Boston, MA. She is an expert on nutrition and physical activity.
- Marian Neuhouser, Ph.D., R.D.: Full Member, Cancer Prevention Program, Division of Public Health Sciences, Fred Hutchinson Cancer Research Center, Seattle, WA. She is a nutritional epidemiologist with broad experience in large clinical trials, including the Women’s Health Initiative and the Prostate Cancer Prevention Trial, small-scale controlled dietary interventions, and large observational cohorts. She has expertise in the role of numerous dietary components in cancer risk, including carbohydrates, dietary fiber, and vitamin D.
- Rafael Pérez-Escamilla, Ph.D.: Professor of Epidemiology and Public Health, Yale School of Public Health. He is an internationally recognized scholar in the area of community nutrition for his work in pregnancy and lactation, food security, obesity, diabetes, and food safety.
- Anna Maria Siega-Riz, Ph.D., R.D.: Professor, Departments of Epidemiology and Nutrition, University of North Carolina at Chapel Hill. Her research has focused on maternal nutritional status and on the dietary patterns among Hispanic adults and children.
- Mary Story, Ph.D., R.D.: Senior Associate Dean for Academic and Student Affairs and Professor, Division of Epidemiology and Community Health, School of Public Health, University of Minnesota. Dr. Story concurrently serves as Director of the National Program Office for the Robert Wood Johnson Foundation Healthy Eating Research Program that supports research on environmental and policy strategies to promote healthy eating among children to prevent childhood obesity.
These are good people. They are bright people. They are people of high integrity. In fact, they were all thoroughly vetted for conflicts of interest before they were appointed to their positions and were required to submit a financial disclosure form annually. The bottom line is that they are all top-flight, mainstream academics and medical professionals and all associated with some of the most prominent and respected institutions in the country. And, yet, therein lies a crushing problem! They are all essentially from the same school of thought. Do you see even one person from the schools of natural health or complementary healing in the group–even one?
And why is this an issue?
Because if everyone comes from the same school of thought, you’ve pretty much confined their collective thinking to a box. Keep in mind that it is people like this–although not necessarily these people in particular–who:
 Denied the connection between diet and cancer for decades.
Denied the connection between diet and cancer for decades.- Denied the connection between trans-fatty acids and heart disease for decades.
- Denied the connection between high glycemic carbs–especially sugar– and diabetes for decades.
- Denied the connection between fast food diets and obesity for decades.
- Denied the connection between low-fiber diets and both colon cancer and diverticular disease for over a century.
- Denied the connection between probiotics and health for decades–in fact, denied ascribing any health value to probiotics for over a century.
- Denied the connection between trace minerals and health for decades–and pretty much still do.
- Denied the connection between organic foods and higher nutrition levels–and, in fact, are still denying it. The trick is in what you measure. If you measure vitamin C and beta carotene, then yes, there is little difference. They are made from carbon, oxygen, and hydrogen–elements that plants can pull from air and water. It doesn’t matter what kind of fertilizer you use or how you treat your soil. But if you start looking at the mineral content in your food, then depleted soils matter because commercial fertilizers contain no minerals to replenish the soil. And if you look at antioxidants, which the plants use to defend themselves against insects and pathogens, you will again notice a huge difference between conventional and organic produce. To put it simply, if you’re dousing plants with herbicides and pesticides that eliminate all potential threats, then the plants have nothing to defend against since the toxic chemicals do it for them and cut back on their own production of antioxidants since they are no longer necessary.
- Deny the difference between synthetic and natural nutrients.
- Etc.
- Etc.
- Etc.
But the problems don’t end there. Even worse, the very methodology they used guaranteed that these issues would never be covered. According to the Guidelines, the Committee used four “state-of-the-art” approaches to review and analyze the available evidence:
- Original systematic reviews
- Existing systematic reviews
- Data analysis
- Food pattern modeling analyses
Unfortunately, as we’ve discussed in other newsletters, once a bias gets embedded in the scientific community, it becomes almost impossible to reverse that bias for decades because new studies cite the original erroneous studies, and then those “new” studies get cited by even newer studies, and on and on so that in a very short time, that erroneous bias becomes established fact. We’ve seen this, for example, where it is now established “fact” that vitamins A and E cause cancer, when the actual fact is that real vitamin A and E were never studied, only the synthetic versions, which are very, very different. What this means is that without an “outside” voice pushing the Committee to look past erroneous assumptions, a review of the existing literature will merely reconfirm the existing errors embedded within.
The result is inevitable, and that’s why it can take decades to correct an erroneous recommendation. As one example, radical mastectomies were the accepted norm for almost 100 years when it came to treating breast cancer, with thousands upon thousands of women being subjected to ever more radical and disfiguring surgeries. But this procedure was never tested; it was merely embedded in medical doctrine as the preferred surgery for breast cancer. Eventually, it fell out of favor when enough studies proved that radical mastectomy proved no more effective than lumpectomy (a derisive term created by the medical establishment to undermine “renegade” doctors they disagreed with). Think about that for a moment. It took a hundred years to overturn an untested, unnecessary, and ultimately invalidated surgery that cruelly disfigured a multitude of women simply because it had become embedded in medical canon.
The Guideline’s Recommendations
According to the Guidelines, a healthy eating pattern includes:
 A variety of vegetables from all of the subgroups–dark green, red and orange, legumes (beans and peas), starchy, and other
A variety of vegetables from all of the subgroups–dark green, red and orange, legumes (beans and peas), starchy, and other- Fruits, especially whole fruits
- Grains, at least half of which are whole grains
- Fat-free or low-fat dairy, including milk, yogurt, cheese, and/or fortified soy beverages
- A variety of protein foods, including seafood, lean meats and poultry, eggs, legumes (beans and peas), and nuts, seeds, and soy products
- Oils
A healthy eating pattern limits:
- Saturated fats and trans fats, added sugars, and sodium
Key Recommendations that are quantitative are provided for several components of the diet that should be limited. According to the committee, these components are of particular public health concern in the United States, and the specified limits can help individuals achieve healthy eating patterns within calorie limits:
- Consume less than 10 percent of calories per day from added sugars
- Consume less than 10 percent of calories per day from saturated fats
- Consume less than 2,300 milligrams (mg) per day of sodium
- If alcohol is consumed, it should be consumed in moderation–up to one drink per day for women and up to two drinks per day for men–and only by adults of legal drinking age.
The Errors in Those Recommendations
Taking them in order:
The first problem is with the grain recommendation. No differentiation is made between low glycemic and high glycemic grains (e.g., pearled barley at 25 and brown rice at 55), between low allergy and high allergy grains (rice vs wheat, e.g.), between incomplete protein and complete protein grains (e.g., wheat vs brown rice, millet, and buckwheat), and for that matter, between no gluten and high gluten grains. And of course, no mention of GMO’s. Keep in mind that the UN’s International Agency for Research on Cancer recently declared that Roundup ready GMO crops, including corn and soy, are “probably” carcinogenic.3 Robin Mesnage, Nicolas Defarge, Gilles-Eric Séralini, et al. “Major Pesticides Are More Toxic to Human Cells Than Their Declared Active Principles.” BioMed Research International. Volume 2014 (2014), Article ID 179691, 8 pages. http://www.hindawi.com/journals/bmri/2014/179691/ , 4 T. Bøhna, M. Cuhraa, T. Traavika, et al. “Compositional differences in soybeans on the market: Glyphosate accumulates in Roundup Ready GM soybeans.” Food Chemistry. Volume 153, 15 June 2014, Pages 207–215. http://www.sciencedirect.com/science/article/pii/S0308814613019201 , 5 Samsel A, Seneff S. “Glyphosate, pathways to modern diseases III: Manganese, neurological diseases, and associated pathologies.” Surg Neurol Int. 2015 Mar 24;6:45. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4392553/ , 6 Kurenbach B, Marjoshi D, Amábile-Cuevas CF, et al. “Sublethal Exposure to Commercial Formulations of the Herbicides Dicamba, 2,4-Dichlorophenoxyacetic Acid, and Glyphosate Cause Changes in Antibiotic Susceptibility in Escherichia coli and Salmonella enterica serovar Typhimurium.” MBio. 2015 Mar 24;6(2). pii: e00009-15. http://mbio.asm.org/content/6/2/e00009-15 , 7 Uren Webster TM, Santos EM. “Global transcriptomic profiling demonstrates induction of oxidative stress and of compensatory cellular stress responses in brown trout exposed to glyphosate and Roundup.” BMC Genomics. 2015 Jan 31;16(1):32. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4318436/
 Next comes the recommendation to eat fat-free and low-fat dairy. There are actually many reasons for not eating fat-free or low-fat dairy–or any dairy for that matter–but one of the most important (assuming that you’re going to eat it) is that most of the vitamins in dairy (D, A, E, and K) are fat soluble. Take the fat out, and you take the vitamins out. Adding synthetic vitamin D2 does not make up the difference. In addition, low-fat milk is loaded with sugar. One cup of 2-percent milk contains 12.3 grams of sugar, more than you’ll find in a Reese’s Peanut Butter Cup.8 David S. Ludwig, Walter C Willett. “Three Daily Servings of Reduced-Fat Milk: An Evidence-Based Recommendation?” JAMA Pediatr. 2013;167(9):788-789. http://archpedi.jamanetwork.com/article.aspx?articleid=1704826 In addition, as far as whole milk contributing to obesity, it’s simply not true. There’s the study of almost 13,000 adolescents published in the Archives of Pediatrics & Adolescent Medicine that found that “skim and 1% milk were associated with weight gain, but dairy fat was not.”9 Berkey CS, Rockett HR, Willett WC, Colditz GA. “Milk, dairy fat, dietary calcium, and weight gain: a longitudinal study of adolescents.” Arch Pediatr Adolesc Med. 2005 Jun;159(6):543-50. http://www.ncbi.nlm.nih.gov/pubmed/15939853 Then there’s the myth that whole milk contributes to heart disease. When you look at the history of heart disease over the last century, you see that as “nutritionists” have pushed people away from the intake of foods high in saturated fat and cholesterol towards low-fat, low-cholesterol foods, heart disease has steadily increased. In fact, recent studies have confirmed that natural, saturated fat consumed in reasonable amounts has nothing to do with heart disease.10 Patty W Siri-Tarino, Qi Sun, Frank B Hu, Ronald M Krauss. “Meta-analysis of prospective cohort studies evaluating the association of saturated fat with cardiovascular disease.” ajcn.2009.27725. http://ajcn.nutrition.org/content/early/2010/01/13/ajcn.2009.27725.full.pdf+html And finally, there is no mention of the health impact of the growth hormones in most commercial dairy products. Look, if you’re going to consume dairy, then make sure it comes from organic, grass fed cows, and that it’s not homogenized.
Next comes the recommendation to eat fat-free and low-fat dairy. There are actually many reasons for not eating fat-free or low-fat dairy–or any dairy for that matter–but one of the most important (assuming that you’re going to eat it) is that most of the vitamins in dairy (D, A, E, and K) are fat soluble. Take the fat out, and you take the vitamins out. Adding synthetic vitamin D2 does not make up the difference. In addition, low-fat milk is loaded with sugar. One cup of 2-percent milk contains 12.3 grams of sugar, more than you’ll find in a Reese’s Peanut Butter Cup.8 David S. Ludwig, Walter C Willett. “Three Daily Servings of Reduced-Fat Milk: An Evidence-Based Recommendation?” JAMA Pediatr. 2013;167(9):788-789. http://archpedi.jamanetwork.com/article.aspx?articleid=1704826 In addition, as far as whole milk contributing to obesity, it’s simply not true. There’s the study of almost 13,000 adolescents published in the Archives of Pediatrics & Adolescent Medicine that found that “skim and 1% milk were associated with weight gain, but dairy fat was not.”9 Berkey CS, Rockett HR, Willett WC, Colditz GA. “Milk, dairy fat, dietary calcium, and weight gain: a longitudinal study of adolescents.” Arch Pediatr Adolesc Med. 2005 Jun;159(6):543-50. http://www.ncbi.nlm.nih.gov/pubmed/15939853 Then there’s the myth that whole milk contributes to heart disease. When you look at the history of heart disease over the last century, you see that as “nutritionists” have pushed people away from the intake of foods high in saturated fat and cholesterol towards low-fat, low-cholesterol foods, heart disease has steadily increased. In fact, recent studies have confirmed that natural, saturated fat consumed in reasonable amounts has nothing to do with heart disease.10 Patty W Siri-Tarino, Qi Sun, Frank B Hu, Ronald M Krauss. “Meta-analysis of prospective cohort studies evaluating the association of saturated fat with cardiovascular disease.” ajcn.2009.27725. http://ajcn.nutrition.org/content/early/2010/01/13/ajcn.2009.27725.full.pdf+html And finally, there is no mention of the health impact of the growth hormones in most commercial dairy products. Look, if you’re going to consume dairy, then make sure it comes from organic, grass fed cows, and that it’s not homogenized.
Then there’s the recommendation to consume soy beverages. Really? As I’ve explained numerous times before, yes, if you eat small amounts of organic, fermented soy, it actually provides substantial health benefits. But if consumed as a primary protein source in unfermented forms — such as soy milk and tofu — its health and safety values are much more suspect. The dangers of soy are not overwhelming, but they cannot be ignored. It is high in allergens11 Christopher T. Cordle. “Soy Protein Allergy: Incidence and Relative Severity.” J. Nutr. May 1, 2004 vol. 134 no. 5 1213S-1219S. http://jn.nutrition.org/content/134/5/1213S.full and high in phytoestrogens.12 Lindsey Konkel. “Could Eating Too Much Soy Be Bad for You?” Scientific American. November 3, 2009. (Accessed 26 Mar 2016.) http://www.scientificamerican.com/article/soybean-fertility-hormone-isoflavones-genistein/ And those issues are progressively amplified the younger you are. Quite simply, soy formula is an abomination. And finally, it should be mentioned that the vast majority of commercially available soy products are made from Roundup ready GMO soy.
Next we come to the recommendation to consume “oils”–just the word “oils” with no elaboration. What about choosing natural oils over refined oils? What about choosing oils high in omega-3 vs omega-6 to help move your diet back closer to the ideal 1:1 or 2:1 ratio necessary for good health? And what about monounsaturated fats such as olive oil, for that matter? In fact, eating the high omega-6 vegetable oils found in your supermarket is a far more likely culprit in heart disease than saturated fats. And really, no mention as to how cooking with oil changes its health profile dramatically–depending on which oil you use and what temperatures you expose it to?
They talk about reducing trans-fats, but with no mention of the distinction between artificial trans-fats and natural-trans fats. Not all trans-fats are bad. Some natural trans-fats such as CLA, which is found in breast milk,13 Moutsioulis AA, Rule DC, Murrieta CM, et al. “Human breast milk enrichment in conjugated linoleic acid after consumption of a conjugated linoleic acid-rich food product: a pilot study.” Nutr Res. 2008 Jul;28(7):437-42. http://www.ncbi.nlm.nih.gov/pubmed/19083443 are actually necessary for good health.
When recommending the reduced consumption of sugars, no mention is made of what happens to your health if you switch to artificial sweeteners, which is what most people turn to when they are looking to avoid sugar. Aspartame and sucralose14 Scientific Committee On Food “Opinion of the Scientific Committee on Food on sucralose” European Commission Health & Consumer Protection Directorate-General. 12/9/2000. (Accessed 26 Ma3 2016.) http://ec.europa.eu/food/fs/sc/scf/out68_en.pdf are both profoundly harmful to your health.
As for sodium, the issue is far more nuanced than, “keep it under 2300 mg a day.” Natural, unrefined salt does not present the same issues as refined table salt. One reason is that the more potassium you have in your diet, the more sodium you can have without any negative health consequences. Not surprisingly, natural sources of unrefined salt contain potassium; whereas refined salt does not.
What Never Even Got Considered in the Recommendations
And then there are the issues that never even got covered in the report:
- Organic vs conventional. We’ve already talked about the higher nutrition level in organic (when you look for the right things), but there’s also the issue of residual pesticides.
- Fish: farmed vs wild.
- Meat: grass fed vs grain fed. Quite simply, the fat profile of grass fed beef approaches the ideal 1:1 to 2:1 omega-6 to omega-3 ratio your body needs, whereas grain fed beef mirrors the highly unhealthy 30:1 to 50:1 ratios of the grains used to fatten the cattle. And then of course, there are the huge health issues associated with processed meat.
- Heavy metals–other than one incidental mention of mercury when discussing seafood.
- The role of supplements–other than one statement that says, “In some cases, fortified foods and dietary supplements may be useful in providing one or more nutrients that otherwise may be consumed in less than recommended amounts.”15 http://health.gov/dietaryguidelines/2015/guidelines/chapter-1/healthy-eating-patterns/
- Probiotics and fermented foods
- Water: how much to drink, when to drink (not with food as it dilutes digestive juices), and what pH to drink it at.
- pH. An abundance of acid forming foods lowers pH throughout your body (except your blood), which leads to disease states. Consuming more alkaline forming foods in your diet improves your health as well as your immune system.
Conclusion
The bottom line when it comes to how much attention you want to pay to these Guidelines is: what is the track record of the Guidelines over the years? Or to put it another way, how well has the health of the American people been maintained under the stewardship of these nutritional experts and their predecessors in the academic and medical communities?
And the answer is–even as stated in the Guidelines–not very well.
Consider.
Heart Disease
Look at the trend line for heart disease and deaths from heart disease over the last hundred years, and you can see that it has not just gone up but absolutely soared!
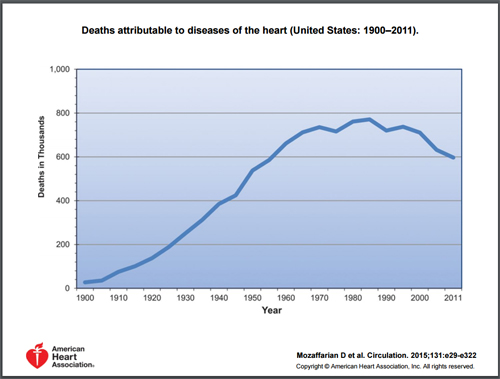
And although mortality rates have dropped a bit over the last couple of decades as the result of medical intervention, the incidence of heart disease has continued unabated. Even as previous guidelines pushed people away from saturated fats into new supposedly “safe” alternatives, rates continued to climb. Why is that? Because the new “safe” alternatives were margarines and shortenings that were low in saturated fats but high in man-made, trans-fatty acids. And even as those of us in the alternative health community screamed in protest, we were ignored. It was over 25 years ago that I labeled partially hydrogenated oils (synthetic trans-fats) as the single greatest killer in the modern diet. It was not until a good 15-20 years later that mainstream nutritionists started getting onboard–without a single apology for the hundreds of thousands–if not millions–of people that they had killed as a result of their earlier recommendations. And now they are pushing high omega-6 vegetable oils that are equally responsible for causing heart disease through their production of non-esterified fatty acids (NEFAs) in the bloodstream.16 Xavier Jouven, Marie-Aline Charles, Michel Desnos, Pierre Ducimetière. “Circulating Nonesterified Fatty Acid Level as a Predictive Risk Factor for Sudden Death in the Population.” Circulation. 2001;104:756-761. http://circ.ahajournals.org/content/104/7/756.full And circulating NEFA concentration in the blood is not just implicated in sudden heart attacks and sudden death, but there is also growing evidence that it’s implicated in the onset of cancer as well! So what exactly are non-esterified fatty acids? In short, NEFAs in the blood are a build-up of excess omega-6 fats in the body, which are caused by eating an overabundance of polyunsaturated fats such as corn, peanut, sunflower, and safflower oils — as recommended in the current guidelines. How many decades and how many deaths will it take until our nutritional stewards come around on this issue too?
Osteoporosis
The incidence of osteoporosis has been steadily climbing for decades. Nutritionists (and the current guidelines) blame that on an aging population and encourage people to eat more calcium rich dairy products to combat the trend, along with calcium “fortified ready-to-eat cereals.”17 http://health.gov/dietaryguidelines/2015/guidelines/appendix-11/ But the incidence of hip fractures (a good indicator of osteoporosis) in countries that have the highest dairy consumption in the world (like Norway, Sweden, and the United States) is 50 times greater than in countries like New Guinea and South Africa that have extremely low consumption of dairy products (and animal products in general).18 Abelow BJ, Holford TR, Insogna KL. “Cross-cultural association between dietary animal protein and hip fracture: a hypothesis.” Calcif Tissue Int. 1992 Jan;50(1):14-8. http://www.ncbi.nlm.nih.gov/pubmed/1739864
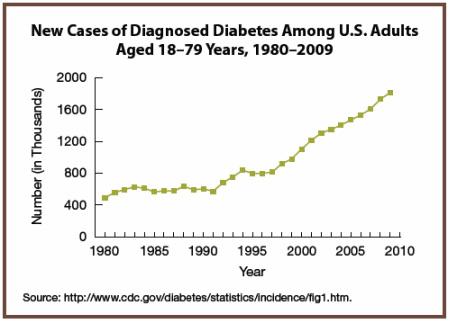
Diabetes
It was back in 1975 that William Duffy wrote Sugar Blues exposing how the high consumption of sugar in the modern diet was behind the increase in a number of major illnesses, including diabetes. At the time, mainstream nutritionists scoffed and called his claims over-the-top hysteria. How wrong they were–yet again. Now, four decades later, the Guidelines recommend eating less sugar. Unfortunately, during that timeframe, the incidence of diabetes in the U.S. has climbed over 400%.
Intestinal Health
Over 100 years ago, John Harvey Kellogg established the Battle Creek Sanitarium that promoted the virtues of intestinal health. Among other things, he advocated the importance of high-fiber foods and beneficial bacteria in the diet, as well as colon cleanses and enemas. Needless to say, mainstream medicine and mainstream nutritionists mocked his ideas–for a hundred years, before finally getting onboard. It’s probably not worth thinking about how many millions of people died from colon cancer or suffered from diverticular disease before doctors and mainstream nutritionists changed their positions–especially considering that, according to the Merck Manual, virtually everyone who eats a modern diet will get diverticular disease if they live long enough.19 Diverticulosis.” The Merck Manual Home Edition. Last full review/revision August 2013 by Michael C. DiMarino, MD. (Accessed 18 Nov 2014.) http://www.merckmanuals.com/home/digestive_disorders/diverticular_disease/diverticulosis.html Oh, and as always, now that they’ve changed positions on fiber and probiotics, did you ever see any acknowledgement that the alternative community was right and they were wrong for decades? In fact, quite the opposite–they pat themselves on the back for their “brand new, groundbreaking discoveries.”
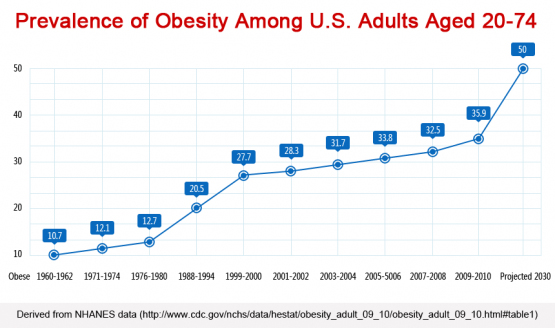
Obesity
Like this really needs any explanation–other than to say, yet again: this worldwide leap into obesity happened on their watch.
To put it simply–based on the above track record–if the people who put together the U.S. Dietary Guidelines worked for a public corporation–based on a simple success vs failure evaluation–they’d have been fired, each and every one of them, long ago. As it stands, since they all work for academia and the medical establishment, where performance doesn’t actually matter since they get to write their own rules of evaluation, they are lauded for their lack of performance and awarded advanced degrees and new administrative positions. Which allows the nonsense to continue!
Final Thoughts
The bottom line is that it’s up to you. Knowing that the establishment tends to run 30-50 years behind the curve, why would you pay attention to anything they recommend–at least until they start bringing in some alternative health experts to help them think outside the box and actually start promoting real health?

References
| ↑1 | “Dietary Guidelines for Americans 2015-2020 Eight Edition.” Office of Disease Prevention and Health Promotion, U.S. Department of Health and Human Services. http://health.gov/dietaryguidelines/2015/guidelines/ |
|---|---|
| ↑2 | “Chronic Disease Prevention and Health Promotion.” CDC. Last updated February 23, 2016. (Accessed 23 Mar 2016.) http://www.cdc.gov/chronicdisease/overview/ |
| ↑3 | Robin Mesnage, Nicolas Defarge, Gilles-Eric Séralini, et al. “Major Pesticides Are More Toxic to Human Cells Than Their Declared Active Principles.” BioMed Research International. Volume 2014 (2014), Article ID 179691, 8 pages. http://www.hindawi.com/journals/bmri/2014/179691/ |
| ↑4 | T. Bøhna, M. Cuhraa, T. Traavika, et al. “Compositional differences in soybeans on the market: Glyphosate accumulates in Roundup Ready GM soybeans.” Food Chemistry. Volume 153, 15 June 2014, Pages 207–215. http://www.sciencedirect.com/science/article/pii/S0308814613019201 |
| ↑5 | Samsel A, Seneff S. “Glyphosate, pathways to modern diseases III: Manganese, neurological diseases, and associated pathologies.” Surg Neurol Int. 2015 Mar 24;6:45. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4392553/ |
| ↑6 | Kurenbach B, Marjoshi D, Amábile-Cuevas CF, et al. “Sublethal Exposure to Commercial Formulations of the Herbicides Dicamba, 2,4-Dichlorophenoxyacetic Acid, and Glyphosate Cause Changes in Antibiotic Susceptibility in Escherichia coli and Salmonella enterica serovar Typhimurium.” MBio. 2015 Mar 24;6(2). pii: e00009-15. http://mbio.asm.org/content/6/2/e00009-15 |
| ↑7 | Uren Webster TM, Santos EM. “Global transcriptomic profiling demonstrates induction of oxidative stress and of compensatory cellular stress responses in brown trout exposed to glyphosate and Roundup.” BMC Genomics. 2015 Jan 31;16(1):32. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4318436/ |
| ↑8 | David S. Ludwig, Walter C Willett. “Three Daily Servings of Reduced-Fat Milk: An Evidence-Based Recommendation?” JAMA Pediatr. 2013;167(9):788-789. http://archpedi.jamanetwork.com/article.aspx?articleid=1704826 |
| ↑9 | Berkey CS, Rockett HR, Willett WC, Colditz GA. “Milk, dairy fat, dietary calcium, and weight gain: a longitudinal study of adolescents.” Arch Pediatr Adolesc Med. 2005 Jun;159(6):543-50. http://www.ncbi.nlm.nih.gov/pubmed/15939853 |
| ↑10 | Patty W Siri-Tarino, Qi Sun, Frank B Hu, Ronald M Krauss. “Meta-analysis of prospective cohort studies evaluating the association of saturated fat with cardiovascular disease.” ajcn.2009.27725. http://ajcn.nutrition.org/content/early/2010/01/13/ajcn.2009.27725.full.pdf+html |
| ↑11 | Christopher T. Cordle. “Soy Protein Allergy: Incidence and Relative Severity.” J. Nutr. May 1, 2004 vol. 134 no. 5 1213S-1219S. http://jn.nutrition.org/content/134/5/1213S.full |
| ↑12 | Lindsey Konkel. “Could Eating Too Much Soy Be Bad for You?” Scientific American. November 3, 2009. (Accessed 26 Mar 2016.) http://www.scientificamerican.com/article/soybean-fertility-hormone-isoflavones-genistein/ |
| ↑13 | Moutsioulis AA, Rule DC, Murrieta CM, et al. “Human breast milk enrichment in conjugated linoleic acid after consumption of a conjugated linoleic acid-rich food product: a pilot study.” Nutr Res. 2008 Jul;28(7):437-42. http://www.ncbi.nlm.nih.gov/pubmed/19083443 |
| ↑14 | Scientific Committee On Food “Opinion of the Scientific Committee on Food on sucralose” European Commission Health & Consumer Protection Directorate-General. 12/9/2000. (Accessed 26 Ma3 2016.) http://ec.europa.eu/food/fs/sc/scf/out68_en.pdf |
| ↑15 | http://health.gov/dietaryguidelines/2015/guidelines/chapter-1/healthy-eating-patterns/ |
| ↑16 | Xavier Jouven, Marie-Aline Charles, Michel Desnos, Pierre Ducimetière. “Circulating Nonesterified Fatty Acid Level as a Predictive Risk Factor for Sudden Death in the Population.” Circulation. 2001;104:756-761. http://circ.ahajournals.org/content/104/7/756.full |
| ↑17 | http://health.gov/dietaryguidelines/2015/guidelines/appendix-11/ |
| ↑18 | Abelow BJ, Holford TR, Insogna KL. “Cross-cultural association between dietary animal protein and hip fracture: a hypothesis.” Calcif Tissue Int. 1992 Jan;50(1):14-8. http://www.ncbi.nlm.nih.gov/pubmed/1739864 |
| ↑19 | Diverticulosis.” The Merck Manual Home Edition. Last full review/revision August 2013 by Michael C. DiMarino, MD. (Accessed 18 Nov 2014.) http://www.merckmanuals.com/home/digestive_disorders/diverticular_disease/diverticulosis.html |








Sadly everything Jon says is
Sadly everything Jon says is true.
Hi Jon,
Hi Jon,
thanks for your well critiqued and informative responses.
I have heard that NASA conducted significant research into so many areas of health and wellbeing as part of their programs for sending astronauts’ into space. If true, there is a significant conflict of interest for what the US government supports via the FDA etc and what they know to be true in reality, based on credible science funded by them! I think much of NASA’s research is accessible. thanks ES
Thank you Jon!
Thank you Jon!
Knowing that the “…primary audiences … are policymakers as well as nutrition and health professionals, not the general public.” helps give some perspective on how to view the “Guidelines”.
I’d like to add to the perspective by saying the only reason why the HHS and USDA produce these “guidelines” is because they are the bastard of corporate food, medical, pharmaceutical and chemical industries.
An impressive array of like
An impressive array of like minded people as you say but i do not know if the answer lies with having alternative medicine people on the panel unless you are saying that alternative medicine people do better science or make better conclusions because of what. All that I have seen of factual alternative opinions has been based on actual scientific studies done by scientific researchers more than likely high academic achievers who have come from the same universities as this panel. Alternative medicine did not do the study the academic researcher did and yet both the alternative medicine and the pharmaceutical are going to read the same paper and yet come up with different theories and therefore solutions but why since none of you did the research. Why does someone have to be labelled alternative or pharmaceutical if he makes and objective observation and thoughtful conclusion. Why not bring out the scientist researchers surely they can tell us and make objective comments or are they to be left out and so we leave it up to the old combatants foes alternative vs allopathic to sought it out and in the end neither one liking or trusting each other. Can we not get a creditable, thoughtful and honest objective analysis without having to label it as alternative.
I think you may have missed
I think you may have missed all of the key points in the article. It was never my intent to claim that “alternative medicine people do better science.” My point was that nutritionists from the alternative health community view the world of diet and health quite differently. They view it based on generations of hands on experience with real people passed down from healer to healer. What they offer is a different viewpoint. How else do you explain the fact that the alternative community identified the importance of fiber and probiotics a century before scientific researchers did–and the dangers of trans fats 50 years before researchers did, etc., etc., etc.
As to the suggestion that scientific researchers would be the best people to determine diet, quite simply, for so many reasons, they would be the worst people to make that judgement. Here’s just a quick sampling.
And I was never suggesting that alternative and allopathics fight it out. All I was suggesting is that people from the alternative community bring thinking that is outside the traditional box. If they were involved and brought their perspective, perhaps we wouldn’t have to wait 50-100 years for every advancement in our understanding of diet and health.
I understand your point but
I understand your point but there is such reliance on science to attempt to describe the possible mechanism which old traditions do not attempt so painstakingly. To be effective i think there is a need for the alternatives to address science to not see themselves as alternatives but as honest rational thinkers in a world that is limited by science funding, honesty, and methodology. I have always thought that the proof that something works is not whether science has been done but whether the person is cured or not and with little to no side affects. Understanding the complete science or mechanisms is like trying to lay down pieces on a jigsaw puzzle which we do not know the size of or shape unless we get enough pieces in one area to make some estimate. I know that you work to bring science into play and that you are a traditionalist but I do not see you as an alternative for doing that if that make sense.
This is by far one of the
This is by far one of the most important and well written articles on health that I have ever read. Every natural health practitioner and individual interested in their health should read this article very carefully and use the information in it to guide all of their future nutritional decisions. I know that I will. Thanks for this wonderful addition to the health and Functional Medicine literature.
Much appreciated. Thank you
Much appreciated. Thank you very much.
I have long been impressed by
I have long been impressed by Jon’s work.
Shared this on fb and hope that others will read, learn and
benefit.